

Blood pressure components and end-stage renal disease in persons with chronic kidney disease: the Kidney Early Evaluation Program (KEEP)
- PMID: 22232147
- PMCID: PMC3417125
- DOI: 10.1001/archinternmed.2011.619
Blood pressure components and end-stage renal disease in persons with chronic kidney disease: the Kidney Early Evaluation Program (KEEP)
Abstract
Background: Treatment of hypertension is difficult in chronic kidney disease (CKD), and blood pressure goals remain controversial. The association between each blood pressure component and end-stage renal disease (ESRD) risk is less well known.
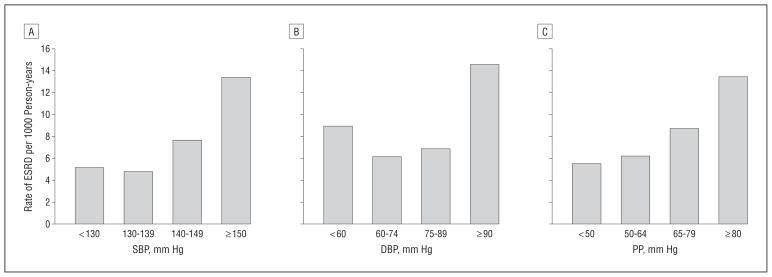
Methods: We studied associations of systolic and diastolic blood pressure (SBP and DBP, respectively) and pulse pressure (PP) with ESRD risk among 16,129 Kidney Early Evaluation Program (KEEP) participants with an estimated glomerular filtration rate of 60 mL/min/1.73 m(2) using Cox proportional hazards. We estimated the prevalence and characteristics associated with uncontrolled hypertension (SBP ≥ 150 or DBP ≥ 90 mm Hg).
Results: The mean (SD) age of participants was 69 (12) years; 25% were black, 6% were Hispanic, and 43% had diabetes mellitus. Over 2.87 years, there were 320 ESRD events. Higher SBP was associated with higher ESRD risk, starting at SBP of 140 mm Hg or higher. After sex and age adjustment, compared with SBP lower than 130 mm Hg, hazard ratios (HRs) were 1.08 (95% CI, 0.74-1.59) for SBP of 130 to 139 mm Hg, 1.72 (95% CI, 1.21-2.45) for SBP of 140 to 149 mm Hg, and 3.36 (95% CI, 2.51-4.49) for SBP of 150 mm Hg or greater. After full adjustment, HRs for ESRD were 1.27 (95% CI, 0.88-1.83) for SBP of 140 to 149 mm Hg and 1.36 (95% CI, 1.02-1.85) for SBP of 150 mm Hg or higher. Persons with DBP of 90 mm Hg or higher were at higher risk for ESRD compared with persons with DBP of 60 to 74 mm Hg (HR, 1.81; 95% CI, 1.33-2.45). Higher PP was also associated with higher ESRD risk (HR, 1.44 [95% CI, 1.00-2.07] for PP ≥ 80 mm Hg compared with PP < 50 mm Hg). Adjustment for SBP attenuated this association. More than 33% of participants had uncontrolled hypertension (SBP ≥ 150 mm Hg or DBP ≥ 90 mm Hg), mostly due to isolated systolic hypertension (54%).
Conclusions: In this large, diverse, community-based sample, we found that high SBP seemed to account for most of the risk of progression to ESRD. This risk started at SBP of 140 mm Hg rather than the currently recommended goal of less than 130 mm Hg, and it was highest among those with SBP of at least 150 mm Hg. Treatment strategies that preferentially lower SBP may be required to improve BP control in CKD.
Figures
Comment in
-
Hypertension: high systolic blood pressure is a major contributor to ESRD risk.Nat Rev Nephrol. 2012 Jan 31;8(3):132. doi: 10.1038/nrneph.2012.10. Nat Rev Nephrol. 2012. PMID: 22290543 No abstract available.
-
What should be the target blood pressure in patients with chronic kidney disease? Data from the Kidney Early Evaluation Program.J Clin Hypertens (Greenwich). 2012 Jul;14(7):472-4. doi: 10.1111/j.1751-7176.2012.00636.x. Epub 2012 Apr 26. J Clin Hypertens (Greenwich). 2012. PMID: 22747621 Free PMC article. No abstract available.
References
-
- Kidney Disease Outcomes Quality Initiative (K/DOQI) K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis. 2004;43(5 suppl 1):S1–S290. - PubMed
-
- Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Stamler J. End-stage renal disease in African-American and white men: 16-year MRFIT findings. JAMA. 1997;277(16):1293–1298. - PubMed
-
- Jafar TH, Stark PC, Schmid CH, et al. AIPRD Study Group. Progression of chronic kidney disease: the role of blood pressure control, proteinuria, and angiotensin-converting enzyme inhibition: a patient-level meta-analysis. Ann Intern Med. 2003;139(4):244–252. - PubMed
-
- Klahr S, Levey AS, Beck GJ, et al. Modification of Diet in Renal Disease Study Group. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. N Engl J Med. 1994;330(13):877–884. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
