

11C-PiB imaging of human immunodeficiency virus-associated neurocognitive disorder
- PMID: 22232345
- PMCID: PMC3536500
- DOI: 10.1001/archneurol.2011.761
11C-PiB imaging of human immunodeficiency virus-associated neurocognitive disorder
Abstract
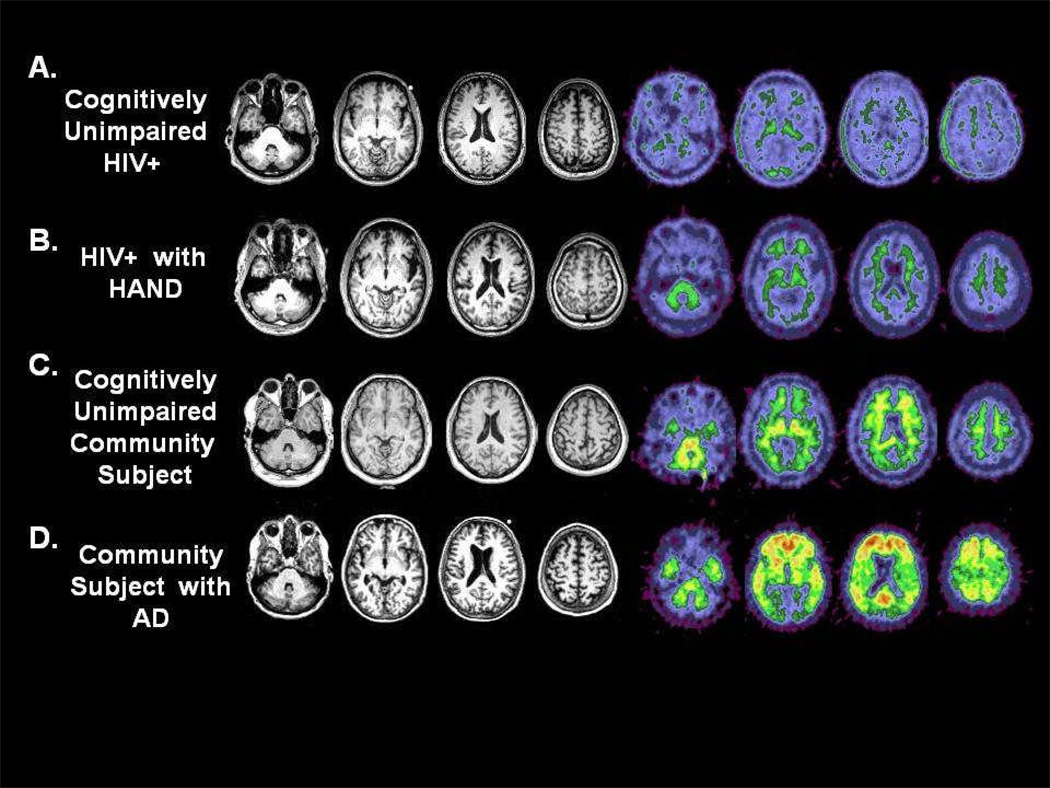
Objective: To evaluate whether the amyloid-binding agent carbon 11-labeled Pittsburgh Compound B ((11)C-PiB) could differentiate Alzheimer disease (AD) from human immunodeficiency virus (HIV)-associated neurocognitive disorder (HAND) in middle-aged HIV-positive participants.
Design: (11)C-PiB scanning, clinical assessment, and cerebrospinal fluid (CSF) analysis were performed. Both χ(2) and t tests assessed differences in clinical and demographic variables between HIV-positive participants and community-living individuals observed at the Knight Alzheimer's Disease Research Center (ADRC). Analysis of variance assessed for regional differences in amyloid-β protein 1-42 (Aβ42) using (11)C-PiB.
Setting: An ADRC and HIV clinic.
Participants: Sixteen HIV-positive participants (11 cognitively normal and 5 with HAND) and 19 ADRC participants (8 cognitively normal and 11 with symptomatic AD).
Main outcome measures: Mean and regional (11)C-PiB binding potentials.
Results: Participants with symptomatic AD were older (P < .001), had lower CSF Aβ42 levels (P < .001), and had higher CSF tau levels (P < .001) than other groups. Regardless of degree of impairment, HIV-positive participants did not have increased (11)C-PiB levels. Mean and regional binding potentials were elevated for symptomatic AD participants (P < .001).
Conclusions: Middle-aged HIV-positive participants, even with HAND, do not exhibit increased (11)C-PiB levels, whereas symptomatic AD individuals have increased fibrillar Aβ42 deposition in cortical and subcortical regions. Observed dissimilarities between HAND and AD may reflect differences in Aβ42 metabolism. (11)C-PiB may provide a diagnostic biomarker for distinguishing symptomatic AD from HAND in middle-aged HIV-positive participants. Future cross-sectional and longitudinal studies are required to assess the utility of (11)C-PiB in older individuals with HAND.
Figures

References
-
- Ances BM, Ellis RJ. Dementia and neurocognitive disorders due to HIV-1 infection. Semin Neurol. 2007 Feb;27(1):86–92. - PubMed
-
- Tozzi V, Corpolongo A, Bellagamba R, Narciso P. Managing patients with sexual transmission of drug-resistant HIV. Sex Health. 2005;2(3):135–142. - PubMed
-
- McArthur JC, Brew BJ. HIV-associated neurocognitive disorders: is there a hidden epidemic? AIDS. Jun 1;24(9):1367–1370. - PubMed
-
- McArthur JC. HIV dementia: an evolving disease. J Neuroimmunol. 2004 Dec;157(1–2):3–10. - PubMed
-
- Sacktor N, Lyles RH, Skolasky R, et al. HIV-associated neurologic disease incidence changes:: Multicenter AIDS Cohort Study, 1990–1998. Neurology. 2001 Jan 23;56(2):257–260. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
