

Multimodality diagnostic imaging in unilateral acute idiopathic maculopathy
- PMID: 22232475
- PMCID: PMC4116109
- DOI: 10.1001/archophthalmol.2011.359
Multimodality diagnostic imaging in unilateral acute idiopathic maculopathy
Abstract
Objective: To describe the clinical features and imaging characteristics in unilateral acute idiopathic maculopathy.
Methods: Retrospective review of 4 patients with a diagnosis of unilateral acute idiopathic maculopathy. Clinical characteristics (age, symptoms, Snellen visual acuity, and funduscopic features) and images from spectral-domain optical coherence tomography, fundus autofluorescence, fluorescein angiography, and indocyanine green angiography were analyzed.
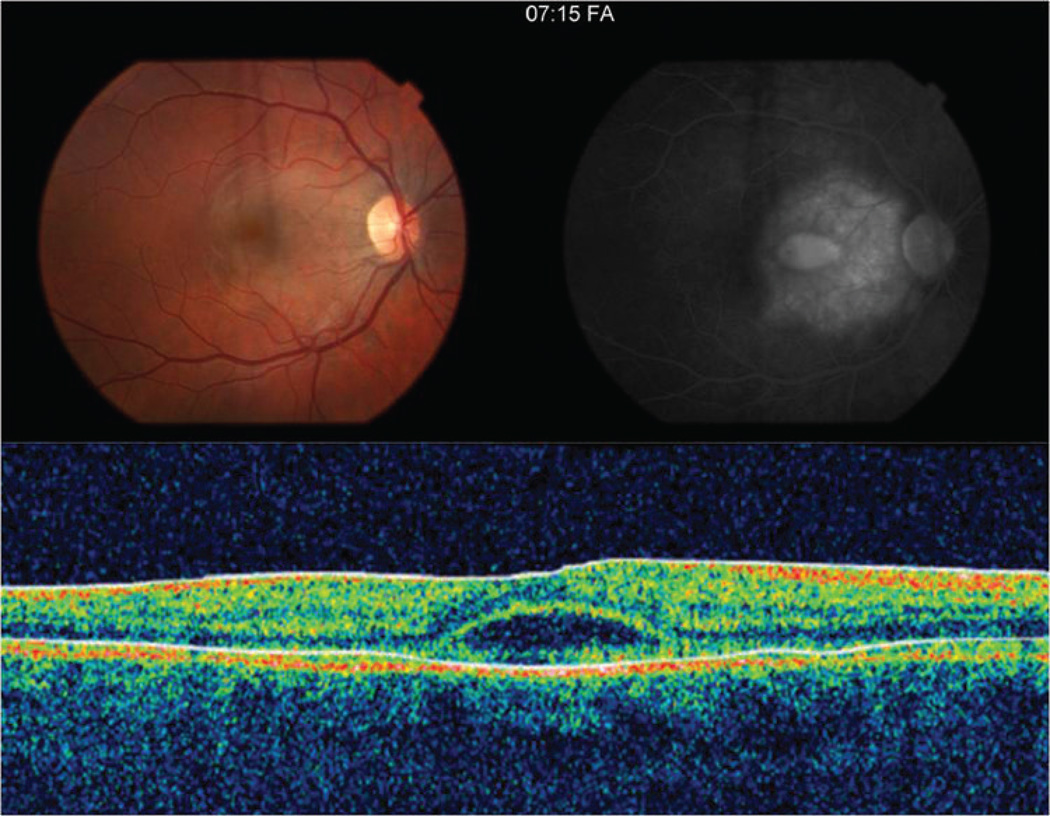
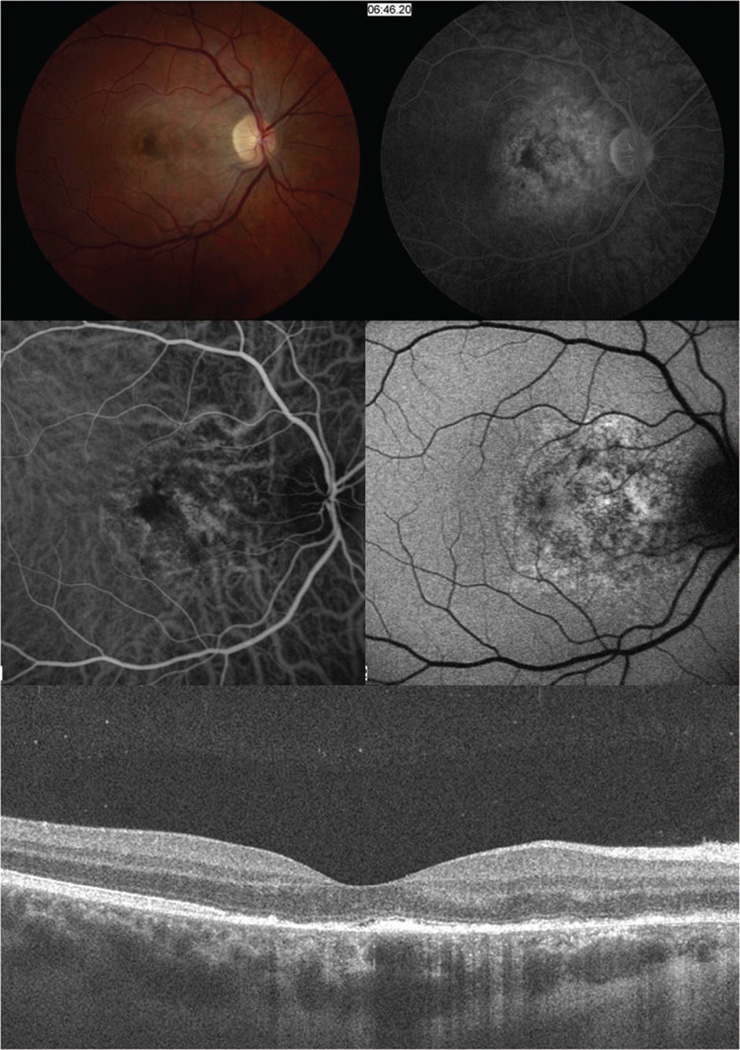
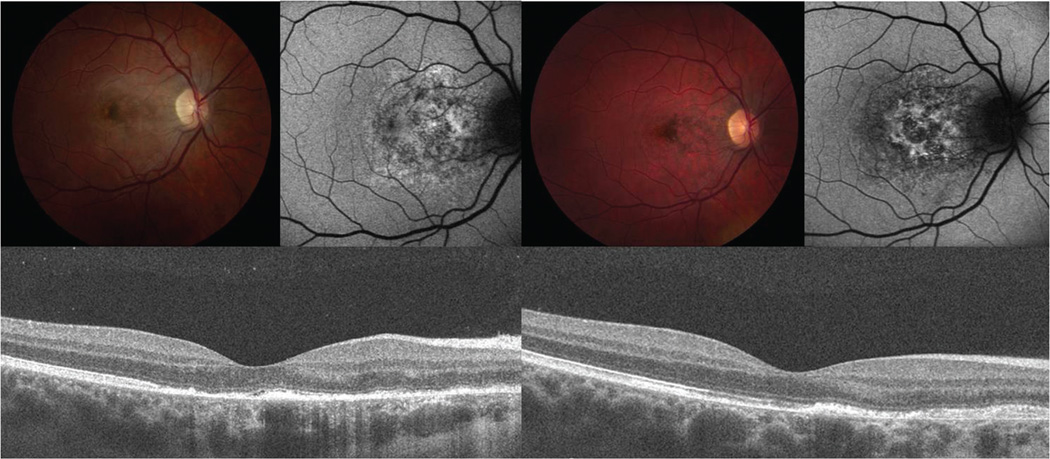
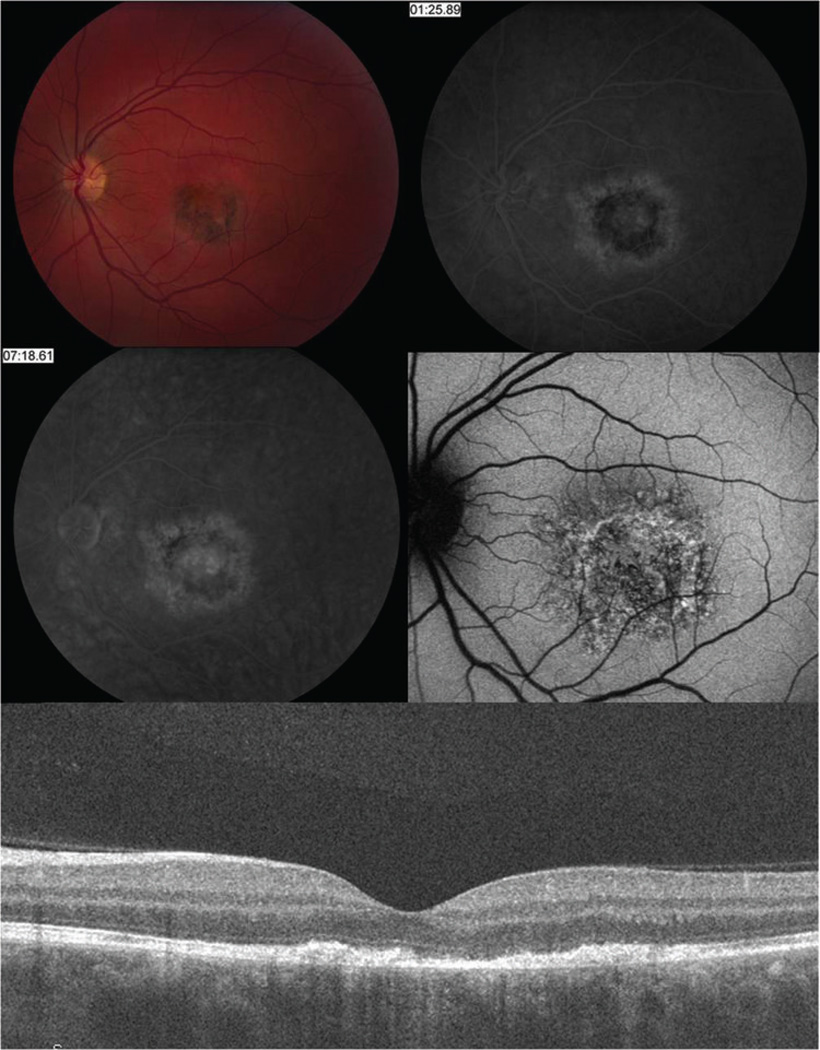
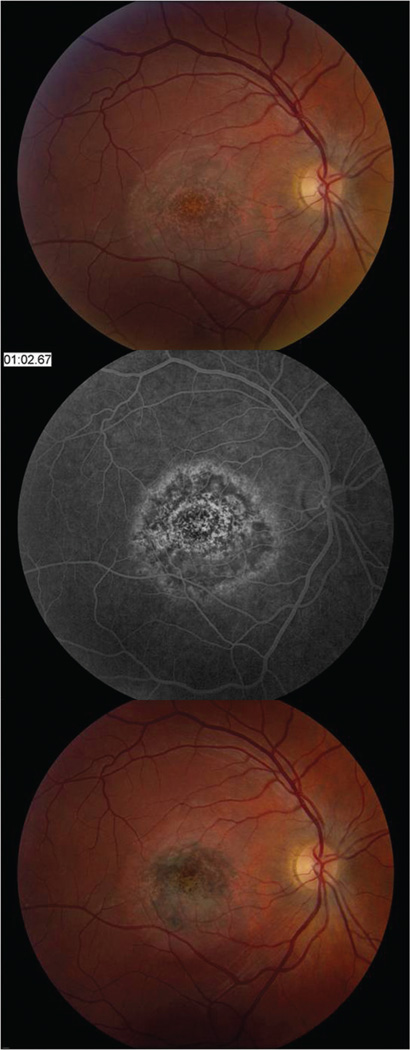
Results: The median (range) age at presentation was 31 (27-52) years. The median (range) interval between symptom onset and presentation was 4 (1-20) weeks. Associated systemic findings included a viral prodrome (50%), orchitis (50%), hand-foot-mouth disease (25%), and positive coxsackievirus titers (50%). The median (range) visual acuity at initial examination was 20/400 (20/70 to 1/400), which improved to 20/30 (20/20 to 20/60) at final follow-up. The median (range) follow-up time was 8 (8-13) weeks. Early in the disease course, the central macula developed irregular, circular areas of white-gray discoloration. Following recovery, the macula had a stippled retinal pigment epithelium characterized by rarefaction and hyperplasia. Fluorescein angiography demonstrated irregular early hyperfluorescence and late subretinal hyperfluorescence. Spectral-domain optical coherence tomography showed a partially reversible disruption of the outer photoreceptor layer. Fundus autofluorescence initially revealed stippled autofluorescence that eventually became more hypoautofluorescent. Indocyanine green angiography showed "moth-eaten"-appearing choroidal vasculature, suggestive of choroidal inflammation.
Conclusions: The imaging characteristics highlight the structural changes during the active and resolution phases of unilateral acute idiopathic maculopathy. The visual recovery correlates with structural changes and suggests that the pathogenesis involves inflammation of the inner choroid, retinal pigment epithelium, and outer photoreceptor complex that is partially reversible.
Figures
References
-
- Yannuzzi LA, Jampol LM, Rabb MF, Sorenson JA, Beyrer C, Wilcox LM. Unilateral acute idiopathic maculopathy. Arch Ophthalmol. 1991;109:1411–1416. - PubMed
-
- Freund KB, Yannuzzi LA, Barile G, Spaide RF, Milewski SA, Guyer DR. The expanding clinical spectrum of unilateral acute idiopathic maculopathy. Arch Ophthalmol. 1996;114:555–559. - PubMed
-
- Day AC, Rotsos T, Holder GE, Tufail A, Robson AG. Electrodiagnostic and two-wavelength fundus autofluorescence imaging investigations in acute idiopathic maculopathy. Doc Ophthalmol. 2010;121:155–160. - PubMed
-
- Haruta H, Sawa M, Saishin Y, Ohguro N, Tano Y. Clinical findings in unilateral acute idiopathic maculopathy. Int Ophthalmol. 2010;30:199–202. - PubMed
-
- Beck AP, Jampol LM, Glasser DA, Florissant M, Pollack JS. Is coxsackievirus the cause of unilateral acute idiopathic maculopathy? Arch Ophthalmol. 2004;122:121–123. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
