

The two pathophysiologies of focal brain ischemia: implications for translational stroke research
- PMID: 22234335
- PMCID: PMC3390813
- DOI: 10.1038/jcbfm.2011.186
The two pathophysiologies of focal brain ischemia: implications for translational stroke research
Abstract
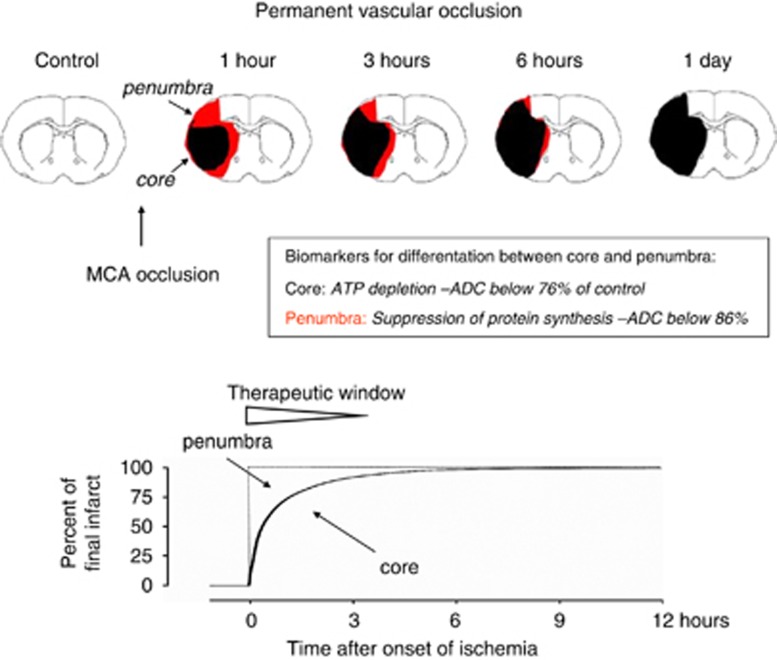
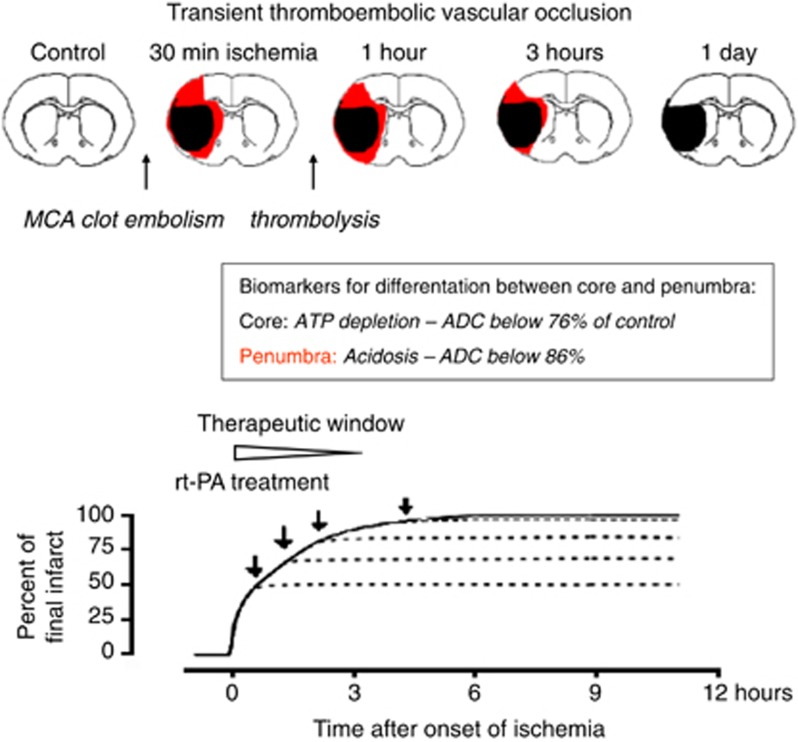
Brain injury after focal ischemia evolves along two basically different pathophysiologies, depending on the severity of the primary flow reduction and the dynamics of postischemic recirculation. In permanent and gradually reversed focal ischemia as after thromboembolic occlusion, primary core injury is irreversible but the expansion of the core into the penumbra can be alleviated by hemodynamic and molecular interventions. Such alleviation can only be achieved within 3 hours after the onset of ischemia because untreated core injury expands to near maximum size during this interval. In promptly reversed transient ischemia as after mechanical vascular occlusion, primary core injury may recover but a secondary delayed injury evolves after a free interval of as long as 6 to 12 hours. This injury can be alleviated throughout the free interval but the longer window is without clinical relevance because transient mechanical vascular occlusion is not a model of naturally occurring stroke. As this difference is widely ignored in stroke research, most clinical trials have been designed with a far too long therapeutic window, which explains their failure. Transient mechanical vascular occlusion models should, therefore, be eliminated from the repertoire of preclinical stroke research.
Figures


References
-
- Astrup J, Symon L, Siesjö BK. Thresholds in cerebral ischemia—The ischemic penumbra. Stroke. 1981;12:723–725. - PubMed
-
- Busch E, Krüger K, Allegrini PR, Kerskens CM, Gyngell ML, Hoehn-Berlage M, Hossmann K-A. Reperfusion after thrombolytic therapy of embolic stroke in the rat: magnetic resonance and biochemical imaging. J Cereb Blood Flow Metab. 1998;18:407–418. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
