

Outcomes of elective total laryngectomy for laryngopharyngeal dysfunction in disease-free head and neck cancer survivors
- PMID: 22235071
- PMCID: PMC4005839
- DOI: 10.1177/0194599811432264
Outcomes of elective total laryngectomy for laryngopharyngeal dysfunction in disease-free head and neck cancer survivors
Abstract
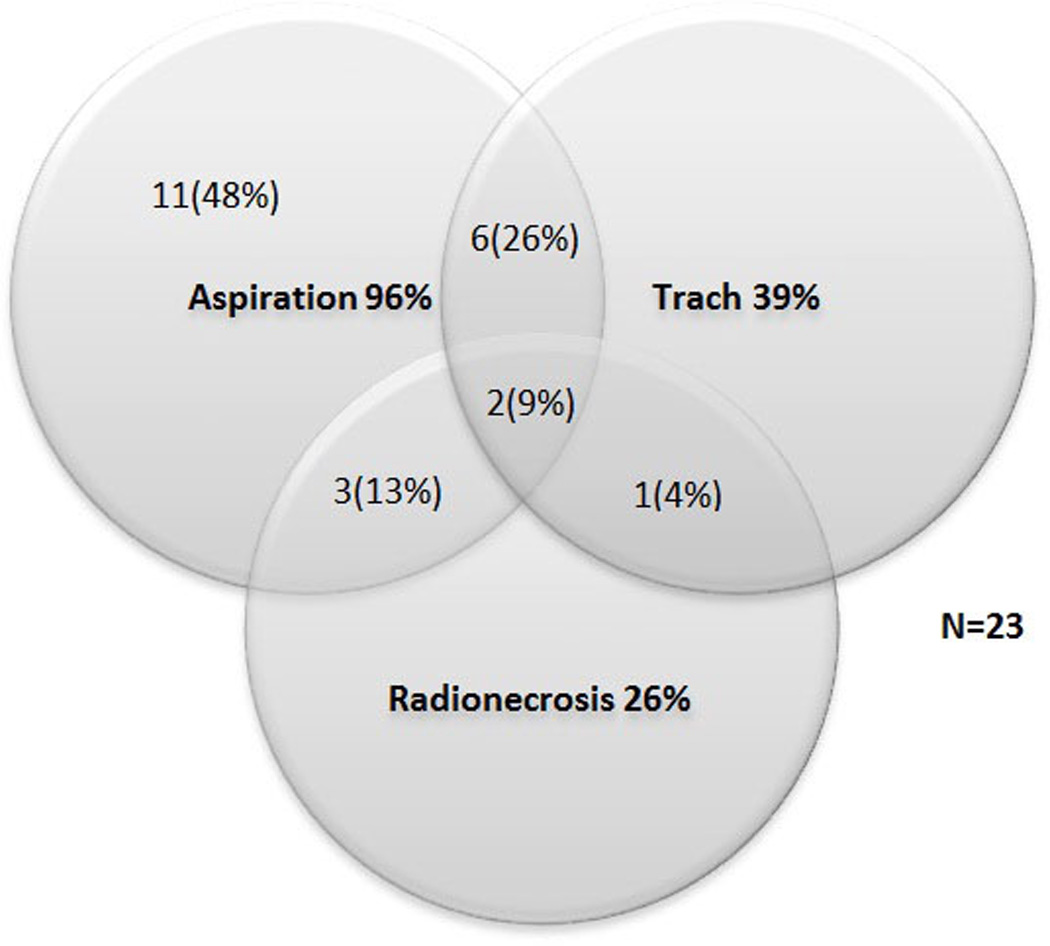
Objective: Total laryngectomy (TL) can be offered for management of chronic aspiration, radionecrosis, and/or airway compromise after head and neck cancer (HNC) treatment. The objective of this study was to evaluate functional outcomes after TL in disease-free HNC survivors.
Design: Retrospective case series with chart review.
Setting: The University of Texas MD Anderson Cancer Center.
Patients: Twenty-three disease-free HNC survivors who underwent TL for laryngopharyngeal dysfunction.
Intervention: TL ± pharyngectomy.
Main outcome measures: Post-TL swallowing-related (diet, gastrostomy dependence, and pneumonia rates) and communication outcomes.
Results: All patients who underwent TL for dysfunction were previously treated with radiotherapy (12/23, 52%) or chemoradiotherapy (11/23, 48%). Preoperative complications included aspiration (22/23, 96%), pneumonia (16/23, 70%), tracheostomy (9/23, 39%), and stricture (7/23, 30%); 17 patients (74%) required enteral/parenteral nutrition, and 13 of 23 (57%) were nothing per oral (NPO). Rates of pneumonia, NPO status, and feeding tube dependence significantly decreased after TL (P < .001). At last follow-up after TL, all patients tolerated oral intake, but 4 (17%) required supplemental enteral nutrition. Continued smoking after radiotherapy and a preoperative history of recurrent pneumonia were significantly (P < .05) associated with final tube dependence and/or diet level. Sixteen patients (70%) underwent tracheoesophageal (TE) puncture, and 57% (13 of 23) communicated using TE voice after TL.
Conclusion: Salvage TL may improve health status by significantly decreasing the rate of pneumonia and improve quality of life by restoring oral intake in patients with refractory laryngopharyngeal dysfunction after HNC treatment. TE voice restoration may enhance functional outcomes in select patients treated with elective TL for dysfunction.
Figures
References
-
- Cooper JS, Porter K, Mallin K, et al. National Cancer Database report on cancer of the head and neck: 10-year update. Head Neck. 2009 Jun;31(6):748–758. - PubMed
-
- Platteaux N, Dirix P, Dejaeger E, Nuyts S. Dysphagia in head and neck cancer patients treated with chemoradiotherapy. Dysphagia. Jun;25(2):139–152. - PubMed
-
- Takano Y, Suga M, Sakamoto O, Sato K, Samejima Y, Ando M. Satisfaction of patients treated surgically for intractable aspiration. Chest. 1999 Nov;116(5):1251–1256. - PubMed
-
- Lazarus C, Logemann JA, Shi G, Kahrilas P, Pelzer H, Kleinjan K. Does laryngectomy improve swallowing after chemoradiotherapy? A case study. Arch Otolaryngol Head Neck Surg. 2002 Jan;128(1):54–57. - PubMed
-
- Garvey CM, Boylan KB, Salassa JR, Kennelly KD. Total laryngectomy in patients with advanced bulbar symptoms of amyotrophic lateral sclerosis. Amyotroph Lateral Scler. 2009 Oct-Dec;10(5–6):470–475. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
