

Association of incident dementia with hospitalizations
- PMID: 22235087
- PMCID: PMC3312921
- DOI: 10.1001/jama.2011.1964
Association of incident dementia with hospitalizations
Abstract
Context: Dementia is associated with increased rates and often poorer outcomes of hospitalization, including worsening cognitive status. New evidence is needed to determine whether some admissions of persons with dementia might be potentially preventable.
Objective: To determine whether dementia onset is associated with higher rates of or different reasons for hospitalization, particularly for ambulatory care-sensitive conditions (ACSCs), for which proactive outpatient care might prevent the need for a hospital stay.
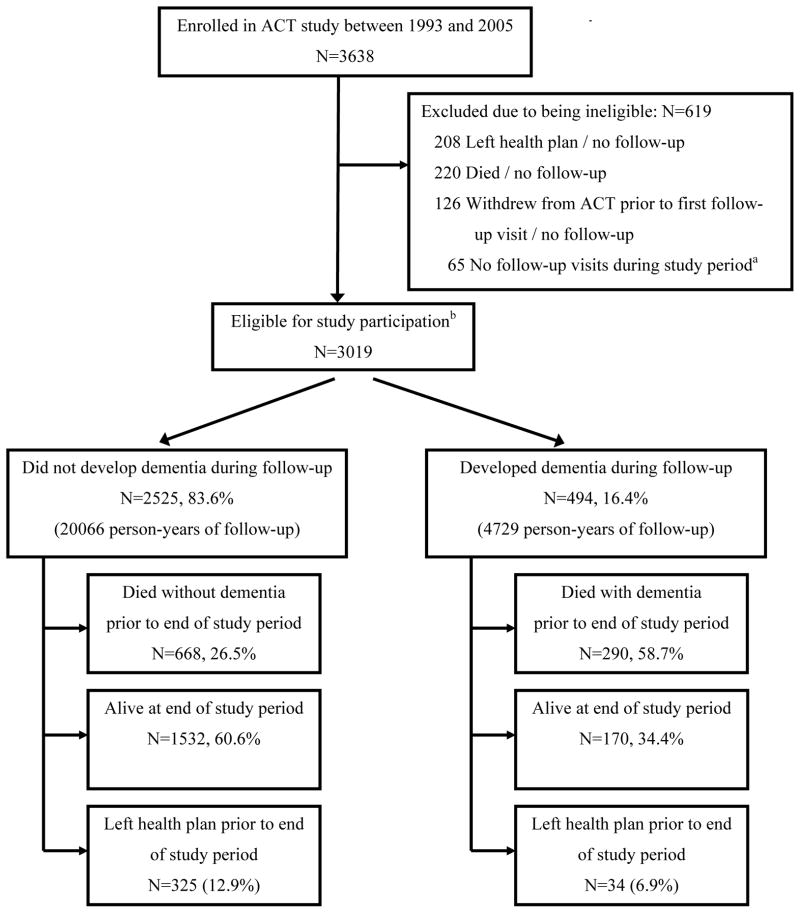
Design, setting, and participants: Retrospective analysis of hospitalizations among 3019 participants in Adult Changes in Thought (ACT), a longitudinal cohort study of adults aged 65 years or older enrolled in an integrated health care system. All participants had no dementia at baseline and those who had a dementia diagnosis during biennial screening contributed nondementia hospitalizations until diagnosis. Automated data were used to identify all hospitalizations of all participants from time of enrollment in ACT until death, disenrollment from the health plan, or end of follow-up, whichever came first. The study period spanned February 1, 1994, to December 31, 2007.
Main outcome measures: Hospital admission rates for patients with and without dementia, for all causes, by type of admission, and for ACSCs.
Results: Four hundred ninety-four individuals eventually developed dementia and 427 (86%) of these persons were admitted at least once; 2525 remained free of dementia and 1478 (59%) of those were admitted at least once. The unadjusted all-cause admission rate in the dementia group was 419 admissions per 1000 person-years vs 200 admissions per 1000 person-years in the dementia-free group. After adjustment for age, sex, and other potential confounders, the ratio of admission rates for all-cause admissions was 1.41 (95% confidence interval [CI], 1.23-1.61; P < .001), while for ACSCs, the adjusted ratio of admission rates was 1.78 (95% CI, 1.38-2.31; P < .001). Adjusted admission rates classified by body system were significantly higher in the dementia group for most categories. Adjusted admission rates for all types of ACSCs, including bacterial pneumonia, congestive heart failure, dehydration, duodenal ulcer, and urinary tract infection, were significantly higher among those with dementia.
Conclusion: Among our cohort aged 65 years or older, incident dementia was significantly associated with increased risk of hospitalization, including hospitalization for ACSCs.
Conflict of interest statement
Figures
Enrolled in ACT between 1993–2005
Free of dementia at time of ACT enrollment
Completed baseline assessment as part of ACT study
At least 1 follow-up visit with ACT to assess dementia status while still enrolled in health plan
Comment in
-
Prevention of unnecessary hospitalization for patients with dementia: the role of ambulatory care.JAMA. 2012 Jan 11;307(2):197-8. doi: 10.1001/jama.2011.2005. JAMA. 2012. PMID: 22235092 No abstract available.
References
-
- Albert SM, Costa R, Merchant C, Small S, Jenders RA, Stern Y. Hospitalization and Alzheimer’s disease: results from a community-based study. J Gerontol A Biol Sci Med Sci. 1999;54(5):M267–271. - PubMed
-
- Lyketsos CG, Sheppard JM, Rabins PV. Dementia in elderly persons in a general hospital. Am J Psychiatry. 2000;157(5):704–707. - PubMed
-
- Bynum JP, Rabins PV, Weller W, Niefeld M, Anderson GF, Wu AW. The relationship between a dementia diagnosis, chronic illness, medicare expenditures, and hospital use. J Am Geriatr Soc. 2004;52(2):187–194. - PubMed
-
- Hill J, Fillit H, Shah SN, del Valle MC, Futterman R. Patterns of healthcare utilization and costs for vascular dementia in a community-dwelling population. J Alzheimers Dis. 2005;8(1):43–50. - PubMed
