

FcγRIIIa expression on monocytes in rheumatoid arthritis: role in immune-complex stimulated TNF production and non-response to methotrexate therapy
- PMID: 22235253
- PMCID: PMC3250404
- DOI: 10.1371/journal.pone.0028918
FcγRIIIa expression on monocytes in rheumatoid arthritis: role in immune-complex stimulated TNF production and non-response to methotrexate therapy
Abstract
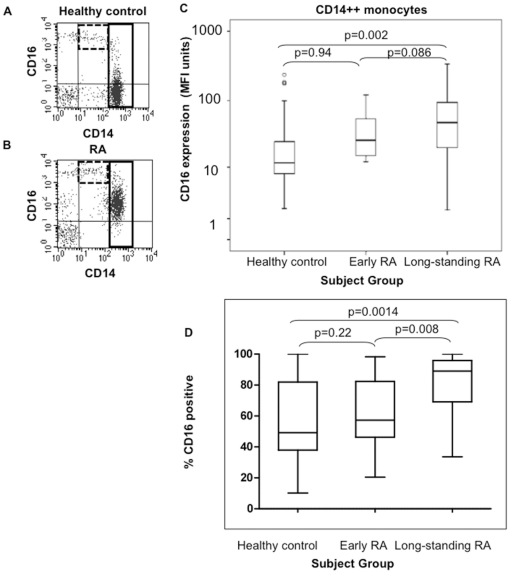
Objective: The expression of FcγRIIIa/CD16 may render monocytes targets for activation by IgG-containing immune complexes (IC). We investigated whether FcγRIIIa/CD16 was upregulated in rheumatoid arthritis (RA), associated with TNF production in response to IC-stimulation, and if this predicted response to methotrexate therapy.
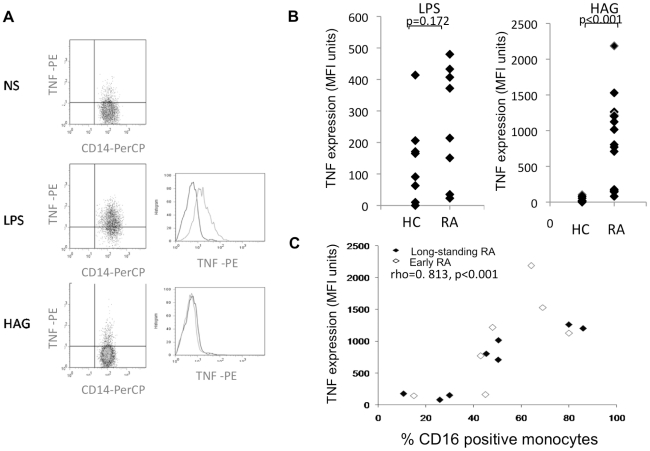
Methods: FcγRIIIa/CD16 expression on CD14(low) and CD14++ monocytes was measured by flow cytometry in healthy controls and RA patients (early and long-standing disease). Intracellular TNF-staining was carried out after in vitro LPS or heat-aggregated immunoglobulin (HAG) activation. FcγRIIIa/CD16 expression pre- and post-steroid/methotrexate treatment was examined.
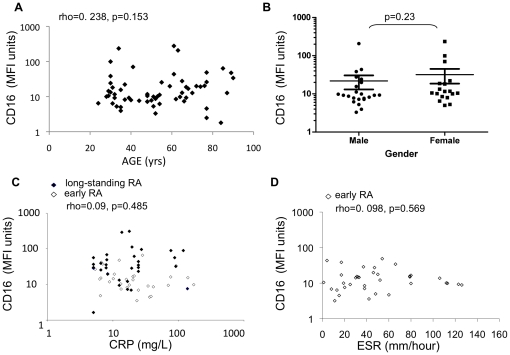
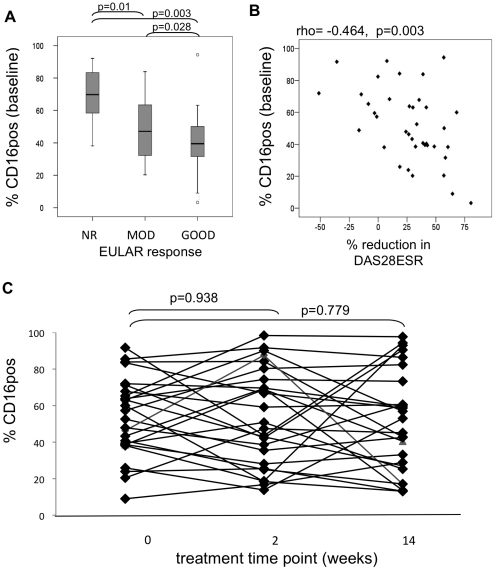
Results: Increased FcγRIIIa/CD16 expression on CD14++ monocytes in long-standing RA patients compared to controls was demonstrated (p = 0.002) with intermediate levels in early-RA patients. HAG-induced TNF-production in RA patients was correlated with the percentage of CD14++ monocytes expressing FcγRIIIa/CD16 (p<0.001). The percentage of CD14++ monocytes expressing FcγRIIIa/CD16 at baseline in early DMARD-naïve RA patients was negatively correlated with DAS28-ESR improvement 14-weeks post-methotrexate therapy (p = 0.003) and was significantly increased in EULAR non-responders compared to moderate (p = 0.01) or good responders (p = 0.003). FcγRIIIa/CD16 expression was not correlated with age, presence of systemic inflammation or autoantibody titers.
Conclusion: Increased FcγRIIIa/CD16 expression on CD14++ monocytes in RA may result in a cell that has increased responsiveness to IC-stimulation. This monocyte subset may contribute to non-response to methotrexate therapy.
Conflict of interest statement
Figures

References
-
- Edwards JCW. Bird HA, Snaith M, editors. Is rheumatoid factor relevant? Questions and uncertainties in rheumatoid arthritis. 1998.
-
- Mewar D, Wilson AG. Autoantibodies in rheumatoid arthritis: a review. Biomed Pharmacother. 2006;60:648–655. - PubMed
-
- Nimmerjahn F, Ravetch JV. Fc-receptors as regulators of immunity. Adv Immunol. 2007;96:179–204. - PubMed
-
- Nimmerjahn F, Ravetch JV. Fc gamma receptors as regulators of immune responses. Nat Rev Immunol. 2008;8:34–47. - PubMed
-
- Dijstelbloem HM, van de Winkel JGJ, Kallenberg CGM. Inflammation in autoimmunity: receptors for IgG revisited. Trends Immunol. 2001;22:510–516. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
