

Considerations for theoretical modelling of thermal ablation with catheter-based ultrasonic sources: implications for treatment planning, monitoring and control
- PMID: 22235787
- PMCID: PMC3366914
- DOI: 10.3109/02656736.2011.630337
Considerations for theoretical modelling of thermal ablation with catheter-based ultrasonic sources: implications for treatment planning, monitoring and control
Abstract
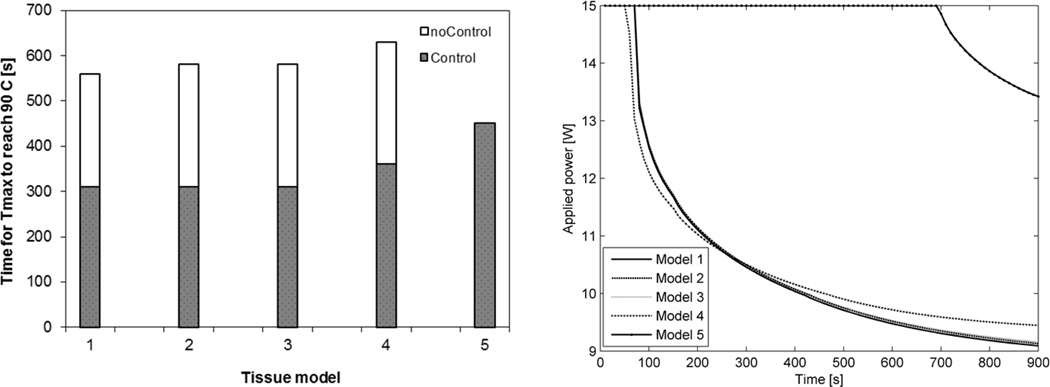
Purpose: To determine the impact of including dynamic changes in tissue physical properties during heating on feedback controlled thermal ablation with catheter-based ultrasound. Additionally, we compared the impact of several indicators of thermal damage on predicted extents of ablation zones for planning and monitoring ablations with this modality.
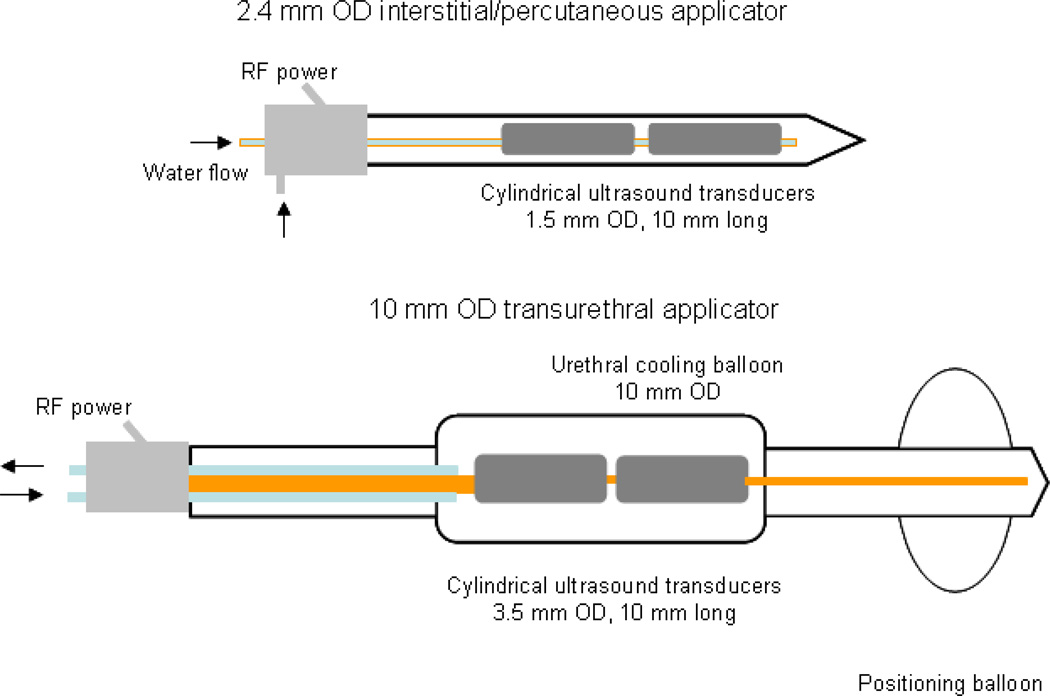
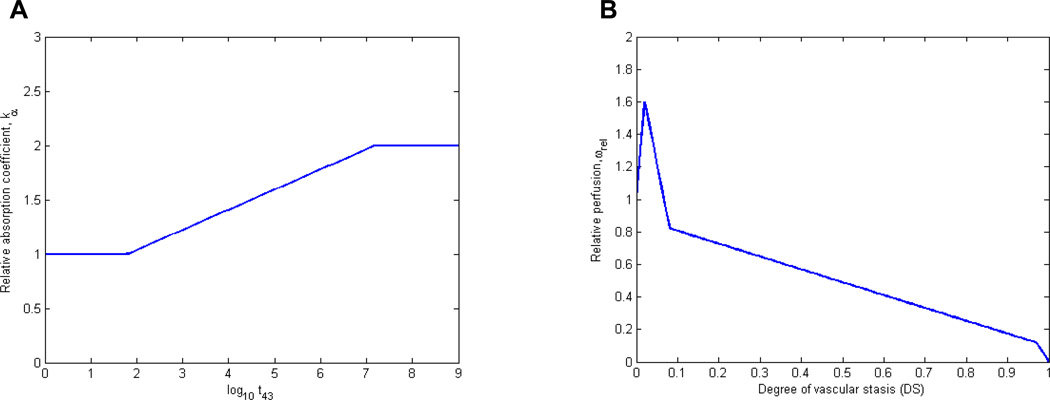
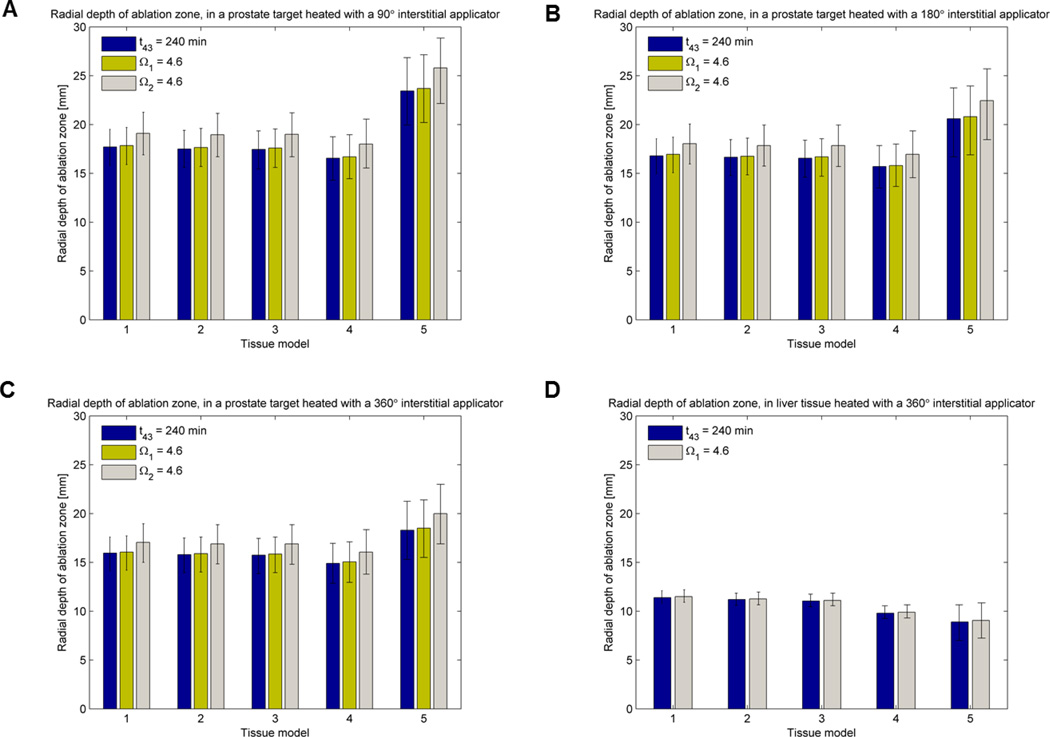
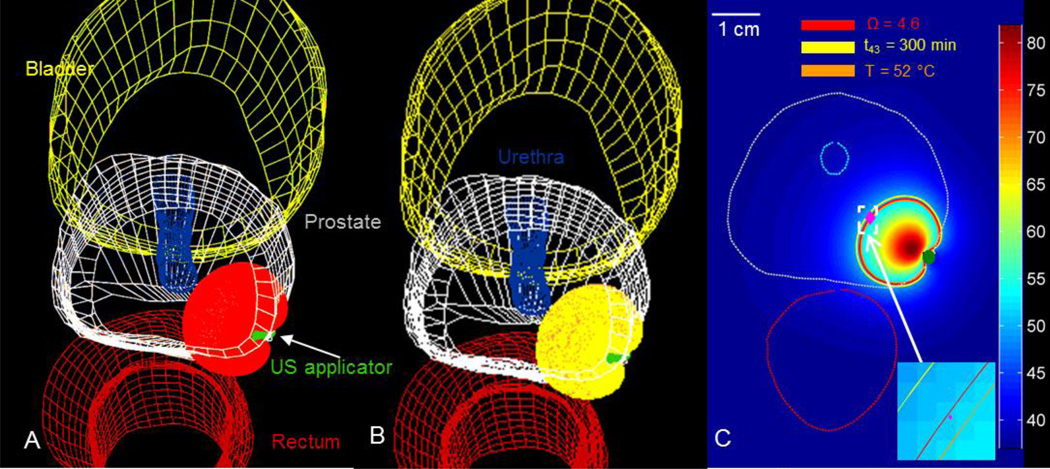
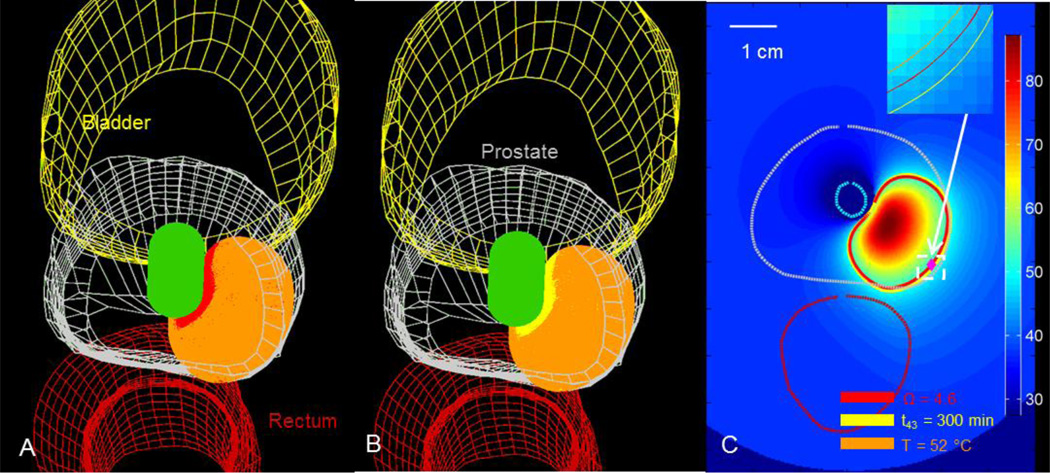
Methods: A 3D model of ultrasound ablation with interstitial and transurethral applicators incorporating temperature-based feedback control was used to simulate thermal ablations in prostate and liver tissue. We investigated five coupled models of heat dependent changes in tissue acoustic attenuation/absorption and blood perfusion of varying degrees of complexity. Dimensions of the ablation zone were computed using temperature, thermal dose, and Arrhenius thermal damage indicators of coagulative necrosis. A comparison of the predictions by each of these models was illustrated on a patient-specific anatomy in the treatment planning setting.
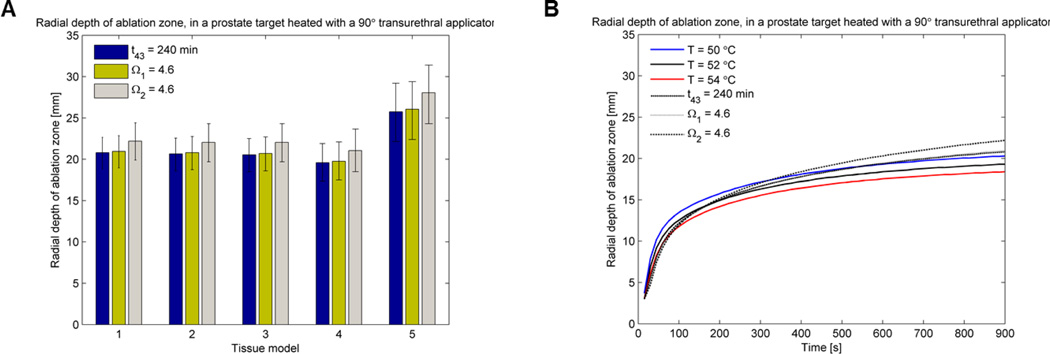
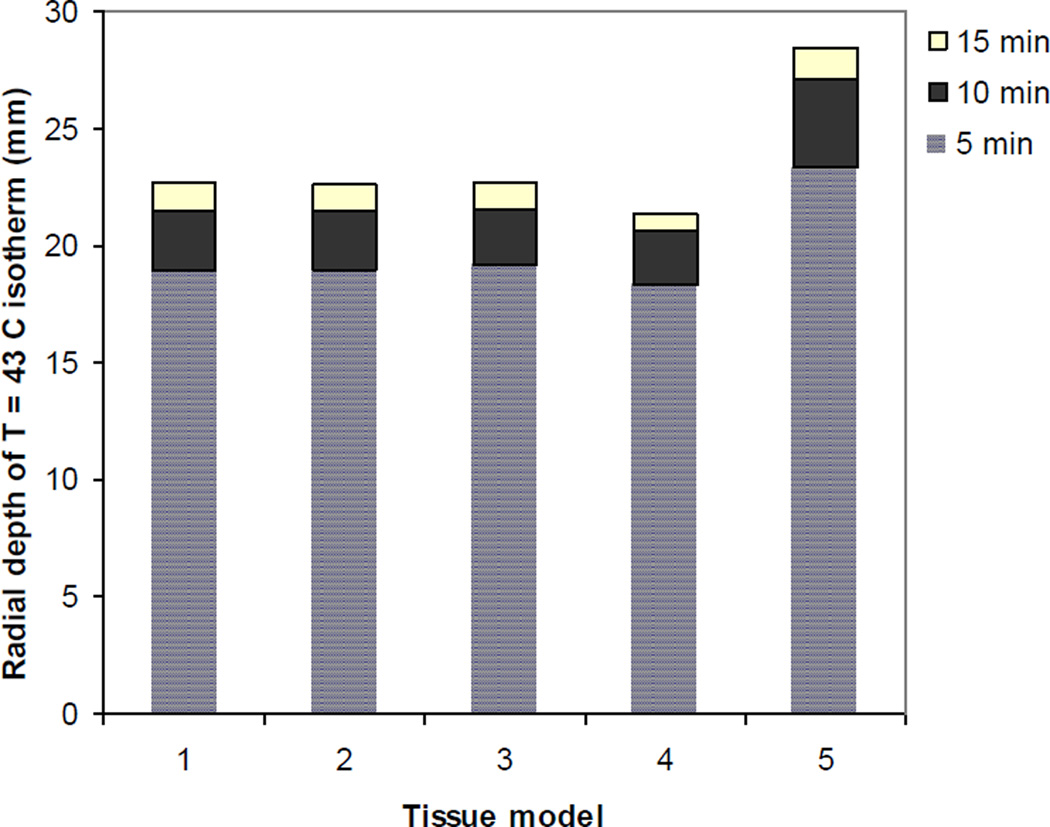
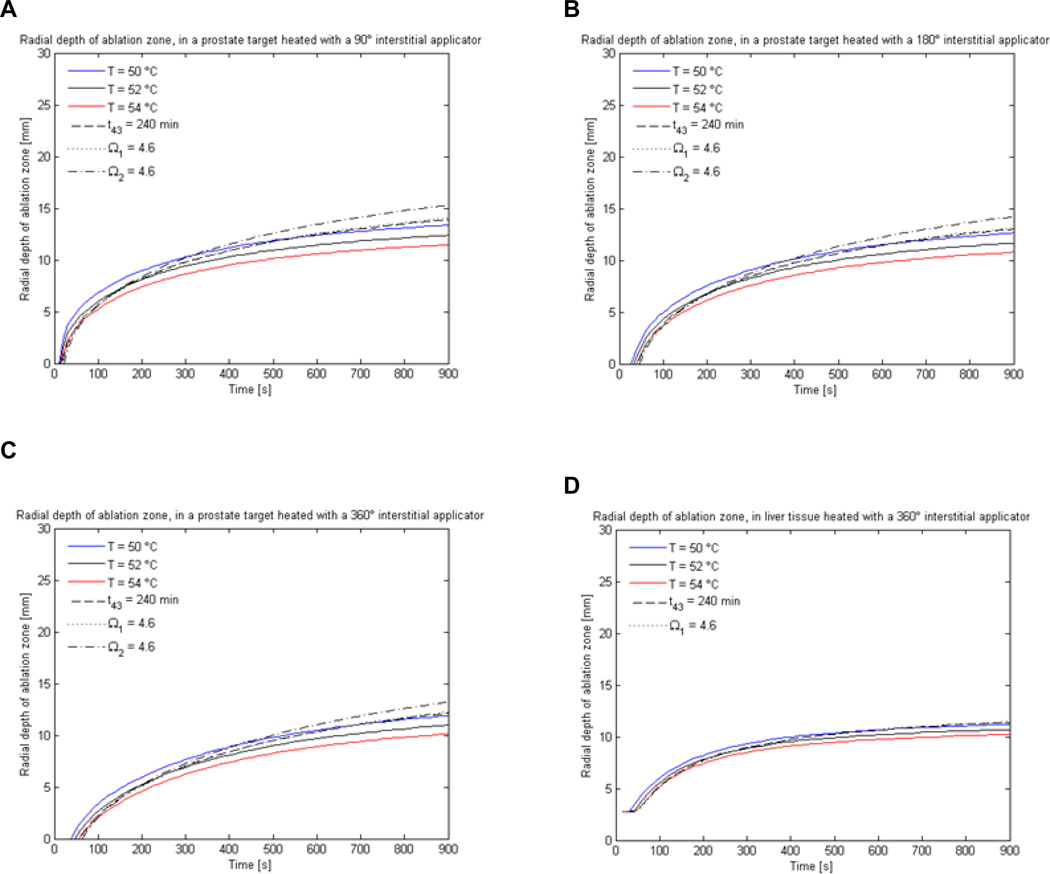
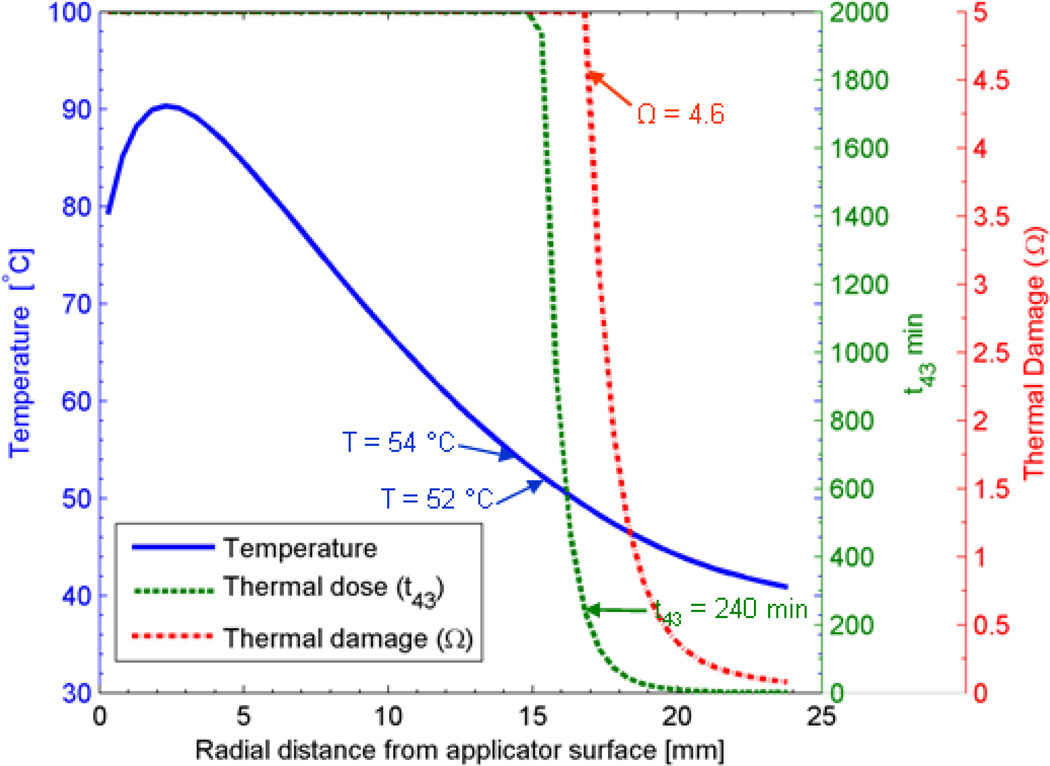
Results: Models including dynamic changes in blood perfusion and acoustic attenuation as a function of thermal dose/damage predicted near-identical ablation zone volumes (maximum variation < 2.5%). Accounting for dynamic acoustic attenuation appeared to play a critical role in estimating ablation zone size, as models using constant values for acoustic attenuation predicted ablation zone volumes up to 50% larger or 47% smaller in liver and prostate tissue, respectively. Thermal dose (t(43) ≥ 240 min) and thermal damage (Ω ≥ 4.6) thresholds for coagulative necrosis are in good agreement for all heating durations, temperature thresholds in the range of 54°C for short (<5 min) duration ablations and 50°C for long (15 min) ablations may serve as surrogates for determination of the outer treatment boundary.
Conclusions: Accounting for dynamic changes in acoustic attenuation/absorption appeared to play a critical role in predicted extents of ablation zones. For typical 5-15 min ablations with this modality, thermal dose and Arrhenius damage measures of ablation zone dimensions are in good agreement, while appropriately selected temperature thresholds provide a computationally cheaper surrogate.
Figures
Similar articles
-
Multiple applicator hepatic ablation with interstitial ultrasound devices: theoretical and experimental investigation.Med Phys. 2012 Dec;39(12):7338-49. doi: 10.1118/1.4765459. Med Phys. 2012. PMID: 23231283 Free PMC article.
-
Modelling of endoluminal and interstitial ultrasound hyperthermia and thermal ablation: applications for device design, feedback control and treatment planning.Int J Hyperthermia. 2013 Jun;29(4):296-307. doi: 10.3109/02656736.2013.800998. Int J Hyperthermia. 2013. PMID: 23738697 Free PMC article. Review.
-
Catheter-based ultrasound applicators for selective thermal ablation: progress towards MRI-guided applications in prostate.Int J Hyperthermia. 2004 Nov;20(7):739-56. doi: 10.1080/02656730410001721816. Int J Hyperthermia. 2004. PMID: 15675669 Review.
-
Catheter-based ultrasound devices and MR thermal monitoring for conformal prostate thermal therapy.Annu Int Conf IEEE Eng Med Biol Soc. 2008;2008:3664-8. doi: 10.1109/IEMBS.2008.4650002. Annu Int Conf IEEE Eng Med Biol Soc. 2008. PMID: 19163505
-
Method for MRI-guided conformal thermal therapy of prostate with planar transurethral ultrasound heating applicators.Phys Med Biol. 2005 Nov 7;50(21):4957-75. doi: 10.1088/0031-9155/50/21/001. Epub 2005 Oct 12. Phys Med Biol. 2005. PMID: 16237234
Cited by
-
Multiple applicator hepatic ablation with interstitial ultrasound devices: theoretical and experimental investigation.Med Phys. 2012 Dec;39(12):7338-49. doi: 10.1118/1.4765459. Med Phys. 2012. PMID: 23231283 Free PMC article.
-
Pancreatic Ductal Adenocarcinoma: Current and Emerging Therapeutic Uses of Focused Ultrasound.Cancers (Basel). 2022 May 24;14(11):2577. doi: 10.3390/cancers14112577. Cancers (Basel). 2022. PMID: 35681557 Free PMC article. Review.
-
Modelling of endoluminal and interstitial ultrasound hyperthermia and thermal ablation: applications for device design, feedback control and treatment planning.Int J Hyperthermia. 2013 Jun;29(4):296-307. doi: 10.3109/02656736.2013.800998. Int J Hyperthermia. 2013. PMID: 23738697 Free PMC article. Review.
-
An endoluminal cylindrical sectored-ring ultrasound phased-array applicator for minimally-invasive therapeutic ultrasound.Med Phys. 2023 Jan;50(1):1-19. doi: 10.1002/mp.16113. Epub 2022 Dec 7. Med Phys. 2023. PMID: 36413363 Free PMC article.
-
Development and validation of a MRgHIFU non-invasive tissue acoustic property estimation technique.Int J Hyperthermia. 2016 Nov;32(7):723-34. doi: 10.1080/02656736.2016.1216184. Epub 2016 Aug 8. Int J Hyperthermia. 2016. PMID: 27441427 Free PMC article.
References
-
- Webb H, Lubner MG, Hinshaw JL. Thermal ablation. Semin Roentgenol. 2011;46(2):133–141. - PubMed
-
- Diederich CJ. Thermal ablation and high-temperature thermal therapy: Overview of technology and clinical implementation. Int J Hyperthermia. 2005;21(8):745–753. - PubMed
-
- Deardorff DL, Diederich CJ, Nau WH. Control of interstitial thermal coagulation: Comparative evaluation of microwave and ultrasound applicators. Med Phys. 2001;28(1):104–117. - PubMed
-
- Mougenot C, Quesson B, de Senneville BD, de Oliveira PL, Sprinkhuizen S, Palussiere J, et al. Three-dimensional spatial and temporal temperature control with mr thermometry-guided focused ultrasound (MRgHIFU) Magn Reson Med. 2009;61(3):603–614. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources