

Impact of comorbidity on colorectal cancer screening cost-effectiveness study in diabetic populations
- PMID: 22237663
- PMCID: PMC3358394
- DOI: 10.1007/s11606-011-1972-6
Impact of comorbidity on colorectal cancer screening cost-effectiveness study in diabetic populations
Abstract
Background: Although comorbidity has been shown to affect the benefits and risks of colorectal cancer (CRC) screening, it has not been accounted for in prior cost-effectiveness analyses of CRC screening.
Objective: To evaluate the impact of diagnosis of diabetes mellitus, a highly prevalent comorbidity in U.S. adults aged 50 and older, on health and economic outcomes of CRC screening.
Design: Cost-effectiveness analysis using an integrated modeling framework.
Data sources: Derived from basic and epidemiologic studies, clinical trials, cancer registries, and a colonoscopy database.
Target population: U.S. 50-year-old population.
Time horizon: Lifetime.
Perspective: Costs are based on Medicare reimbursement rates.
Interventions: Colonoscopy screening at ten-year intervals, beginning at age 50, and discontinued after age 50, 60, 70, 80 or death.
Outcome measures: Health outcomes and cost effectiveness.
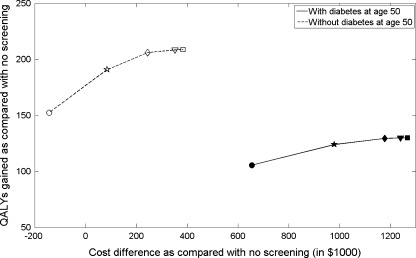
Results of base-case analysis: Diabetes diagnosis significantly affects cost-effectiveness of CRC screening. For the same CRC screening strategy, a person without diabetes at age 50 gained on average 0.07-0.13 life years more than a person diagnosed with diabetes at age 50 or younger. For a population of 1,000 patients diagnosed with diabetes at baseline, increasing stop age from 70 years to 80 years increased quality-adjusted life years (QALYs) gained by 0.3, with an incremental cost-effectiveness ratio of $206,671/QALY. The corresponding figures for 1,000 patients without diabetes are 2.3 QALYs and $46,957/QALY.
Results of sensitivity analysis: Cost-effectiveness results are sensitive to cost of colonoscopy and adherence to colonoscopy screening.
Limitations: Results depend on accuracy of model assumptions.
Conclusion: Benefits of CRC screening differ substantially for patients with and without diabetes. Screening for CRC in patients diagnosed with diabetes at age 50 or younger is not cost-effective beyond age 70. Screening recommendations should be individualized based on the presence of comorbidities.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer Statistics, 2010. CA Cancer J Clin. - PubMed
-
- Atkin WS, Edwards R, Kralj-Hans I, Wooldrage K, Hart AR, Northover JM, et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet;375(9726):1624-33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
