

The 25(OH)D level needed to maintain a favorable bisphosphonate response is ≥33 ng/ml
- PMID: 22237813
- PMCID: PMC3893033
- DOI: 10.1007/s00198-011-1868-7
The 25(OH)D level needed to maintain a favorable bisphosphonate response is ≥33 ng/ml
Abstract
Why only some osteoporotic patients maintain response to prolonged bisphosphonate therapy is unknown. We examined bisphosphonate response and its association with serum 25 hydroxy vitamin D (25(OH)D) level in a "real world" setting. Serum 25(OH)D level was strongly associated with maintaining bisphosphonate response arguing that vitamin D may be involved in optimizing prolonged bisphosphonate therapy.
Introduction: This study examined the maintenance of bisphosphonate response in the "real world" setting and the association between 25(OH)D and bisphosphonate response using an established composite definition of response.
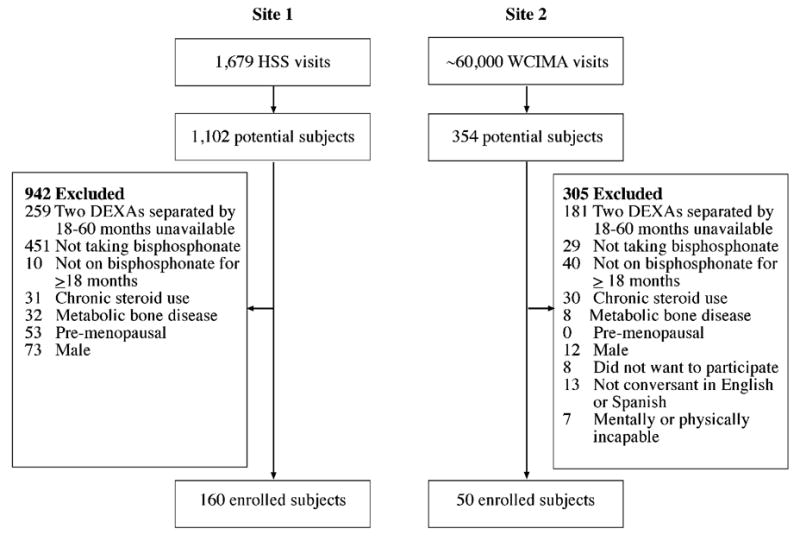
Methods: Postmenopausal women with low bone mineral density (BMD) treated with bisphosphonates were identified from two New York City practices. Patients were excluded for a history of chronic steroid use, metabolic bone disease, or bisphosphonate non-adherence. Patients were categorized as bisphosphonate non-responders if they had a T-score < -3 that persisted between dual-energy X-ray absorptiometry (DEXA) scans, a >3% decrease in BMD, or an incident fracture on bisphosphonate therapy, criteria based on the EUROFORS trial. Demographic and clinical data including mean 25(OH)D levels between DEXA scans were obtained. Mean 25(OH)D levels were compared between responders and non-responders and multiple logistic regression analysis was performed to identify factors associated with non-response.
Results: A total of 210 patients were studied. A favorable response to bisphosphonate therapy was seen in 47% (N = 99/210). Patients with a mean 25(OH)D ≥33 ng/ml had a ~4.5-fold greater odds of a favorable response (P < 0.0001). 25(OH)D level was significantly associated with response - a 1 ng/ml decrease in 25(OH)D was associated with ~5% decrease in odds of responding (odds ratio = 0.95; 95% confidence interval, 0.92-0.98; P = 0.0006).
Conclusions: Patients with a mean 25(OH)D ≥33 ng/ml had a substantially greater likelihood of maintaining bisphosphonate response. This threshold level of 25(OH)D is higher than that considered adequate by the Institute of Medicine, arguing that higher levels may be required for specific therapeutic outcomes.
Conflict of interest statement
We have no conflicts of interest to disclose.
Conflicts of interest: None.
Figures

References
-
- Braithwaite RS, Col NF, Wong JB. Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc. 2003;51:364–370. - PubMed
-
- Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, Bauer DC, Genant HK, Haskell WL, Marcus R, Ott SM, Torner JC, Quandt SA, Reiss TF, Ensrud KE. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet. 1996;348:1535–1541. - PubMed
-
- Black DM, Delmas PD, Eastell R, Reid IR, Boonen S, Cauley JA, Cosman F, Lakatos P, Leung PC, Man Z, Mautalen C, Mesenbrink P, Hu H, Caminis J, Tong K, Rosario-Jansen T, Krasnow J, Hue TF, Sellmeyer D, Eriksen EF, Cummings SR. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med. 2007;356:1809–1822. - PubMed
-
- Black DM, Thompson DE, Bauer DC, Ensrud K, Musliner T, Hochberg MC, Nevitt MC, Suryawanshi S, Cummings SR. Fracture risk reduction with alendronate in women with osteoporosis: the Fracture Intervention Trial. FIT Research Group. J Clin Endocrinol Metab. 2000;85:4118–4124. - PubMed
-
- Harris ST, Watts NB, Genant HK, McKeever CD, Hangartner T, Keller M, Chesnut CH, 3rd, Brown J, Eriksen EF, Hoseyni MS, Axelrod DW, Miller PD. Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA. 1999;282:1344–1352. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
