

Noninferiority of miltefosine versus meglumine antimoniate for cutaneous leishmaniasis in children
- PMID: 22238470
- PMCID: PMC3266136
- DOI: 10.1093/infdis/jir816
Noninferiority of miltefosine versus meglumine antimoniate for cutaneous leishmaniasis in children
Abstract
Background: Children have a lower response rate to antimonial drugs and higher elimination rate of antimony (Sb) than adults. Oral miltefosine has not been evaluated for pediatric cutaneous leishmaniasis.
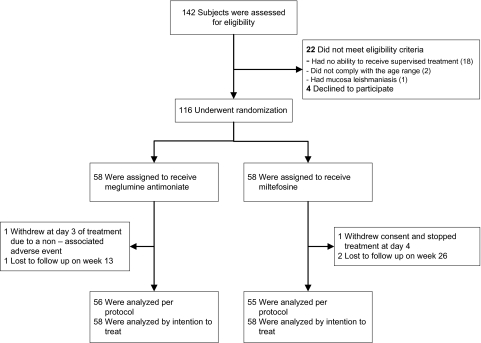
Methods: A randomized, noninferiority clinical trial with masked evaluation was conducted at 3 locations in Colombia where Leishmania panamensis and Leishmania guyanensis predominated. One hundred sixteen children aged 2-12 years with parasitologically confirmed cutaneous leishmaniasis were randomized to directly observed treatment with meglumine antimoniate (20 mg Sb/kg/d for 20 days; intramuscular) (n = 58) or miltefosine (1.8-2.5 mg/kg/d for 28 days; by mouth) (n = 58). Primary outcome was treatment failure at or before week 26 after initiation of treatment. Miltefosine was noninferior if the proportion of treatment failures was ≤15% higher than achieved with meglumine antimoniate (1-sided test, α = .05).
Results: Ninety-five percent of children (111/116) completed follow-up evaluation. By intention-to-treat analysis, failure rate was 17.2% (98% confidence interval [CI], 5.7%-28.7%) for miltefosine and 31% (98% CI, 16.9%-45.2%) for meglumine antimoniate. The difference between treatment groups was 13.8%, (98% CI, -4.5% to 32%) (P = .04). Adverse events were mild for both treatments.
Conclusions: Miltefosine is noninferior to meglumine antimoniate for treatment of pediatric cutaneous leishmaniasis caused by Leishmania (Viannia) species. Advantages of oral administration and low toxicity favor use of miltefosine in children.
Clinical trial registration: NCT00487253.
Figures
References
-
- Campbell-Lendrum D, Dujardin JP, Martinez E, et al. Domestic and peridomestic transmission of American cutaneous leishmaniasis: changing epidemiological patterns present new control opportunities. Mem Inst Oswaldo Cruz. 2001;96:159–62. - PubMed
-
- Munoz G, Davies CR. Leishmania panamensis transmission in the domestic environment: the results of a prospective epidemiological survey in Santander, Colombia. Biomedica. 2006;26(Suppl 1):131–44. - PubMed
-
- Urbanization: an increasing risk factor for leishmaniasis. Wkly Epidemiol Rec. 2002;77:365–70. - PubMed
-
- Yadon ZE, Rodrigues LC, Davies CR, Quigley MA. Indoor and peridomestic transmission of American cutaneous leishmaniasis in northwestern Argentina: a retrospective case-control study. Am J Trop Med Hyg. 2003;68:519–26. - PubMed
-
- Rodriguez-Barraquer I, Gongora R, Prager M, et al. Etiologic agent of an epidemic of cutaneous leishmaniasis in Tolima, Colombia. Am J Trop Med Hyg. 2008;78:276–82. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
