

Simultaneous right and left heart real-time, free-breathing CMR flow quantification identifies constrictive physiology
- PMID: 22239888
- PMCID: PMC4560101
- DOI: 10.1016/j.jcmg.2011.07.010
Simultaneous right and left heart real-time, free-breathing CMR flow quantification identifies constrictive physiology
Abstract
Objectives: The purpose of this study was to evaluate the ability of a novel cardiac magnetic resonance (CMR) real-time phase contrast (RT-PC) flow measurement technique to reveal the discordant respirophasic changes in mitral and tricuspid valve in flow indicative of the abnormal hemodynamics seen in constrictive pericarditis (CP).
Background: Definitive diagnosis of CP requires identification of constrictive hemodynamics with or without pericardial thickening. CMR to date has primarily provided morphological assessment of the pericardium.
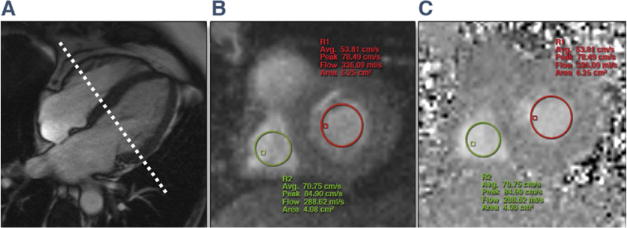
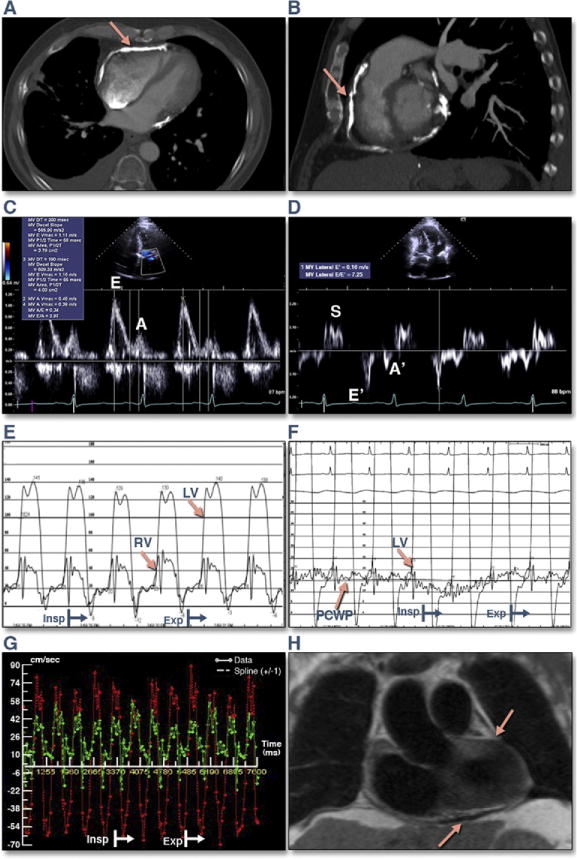
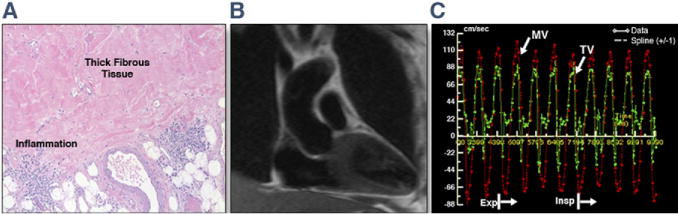
Methods: Sixteen patients (age 57 ± 13 years) undergoing CMR to assess known or suspected CP and 10 controls underwent RT-PC that acquired simultaneous mitral valve and tricuspid valve inflow velocities over 10 s of unrestricted breathing. The diagnosis of CP was confirmed via clinical history, diagnostic imaging, cardiac catheterization, intraoperative findings, and histopathology.
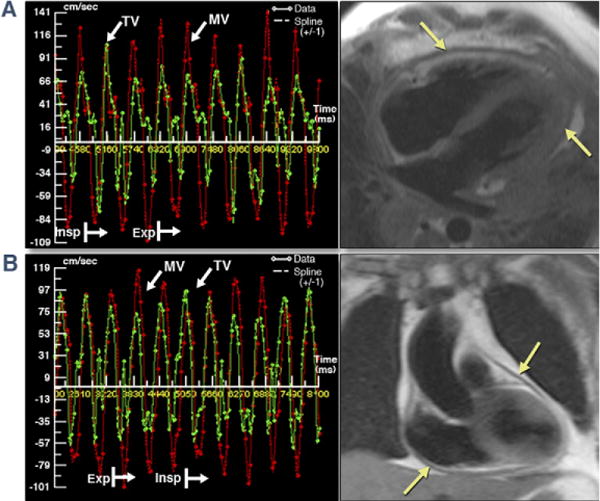
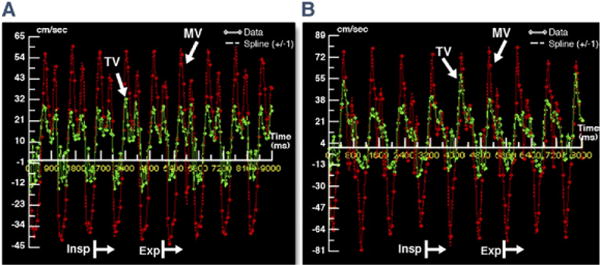
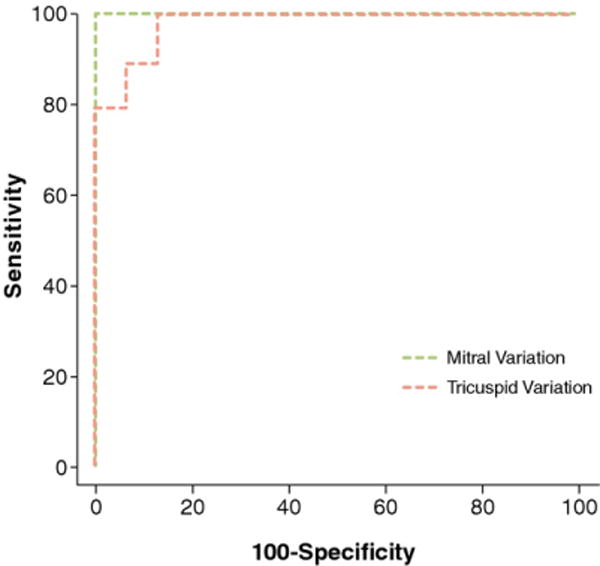
Results: Ten patients had CP, all with increased pericardial thickness (6.2 ± 1.0 mm). RT-PC imaging demonstrated discordant respirophasic changes in atrioventricular valve inflow velocities in all CP patients, with mean ± SD mitral valve and tricuspid valve inflow velocity variation of 46 ± 20% and 60 ± 15%, respectively, compared with 16 ± 8% and 24 ± 11% in patients without CP (p < 0.004 vs. patients with CP for both) and 17 ± 5% and 31 ± 13% in controls (p < 0.001 vs. patients with CP for both). There was no difference in atrioventricular valve inflow velocity variation between patients without CP compared with controls (p > 0.3 for both). Respiratory variation exceeding 25% across the mitral valve yielded a sensitivity of 100%, a specificity of 100%, and an area under the receiver-operating characteristic curve of 1.0 to detect CP physiology. Using a cutoff of 45%, variation of transtricuspid valve velocity had a sensitivity of 90%, a specificity of 88%, and an area under the receiver-operating characteristic curve of 0.98.
Conclusions: Accentuated and discordant respirophasic changes in mitral valve and tricuspid valve inflow velocities characteristic of CP can be identified noninvasively with RT-PC CMR. When incorporated into existing CMR protocols for imaging pericardial morphology, RT-PC CMR provides important hemodynamic evidence with which to make a definite diagnosis of CP.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
CMR imaging for diastolic hemodynamic assessment fantasy or reality?JACC Cardiovasc Imaging. 2012 Jan;5(1):25-7. doi: 10.1016/j.jcmg.2011.08.018. JACC Cardiovasc Imaging. 2012. PMID: 22239889 No abstract available.
References
-
- McCaughan BC, Schaff HV, Piehler JM, et al. Early and late results of pericardiectomy for constrictive pericarditis. J Thorac Cardiovasc Surg. 1985;89:340–50. - PubMed
-
- Verhaert D, Gabriel RS, Johnston D, Lytle BW, Desai MY, Klein AL. The role of multimodality imaging in the management of pericardial disease. Circ Cardiovasc Imaging. 2010;3:333–43. - PubMed
-
- Yared K, Baggish AL, Picard MH, Hoffmann U, Hung J. Multimodality imaging of pericardial diseases. J Am Coll Cardiol Img. 2010;3:650–60. - PubMed
-
- Talreja DR, Edwards WD, Danielson GK, et al. Constrictive pericarditis in 26 patients with histologically normal pericardial thickness. Circulation. 2003;108:1852–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
