

Correlation between arterial FDG uptake and biomarkers in peripheral artery disease
- PMID: 22239891
- PMCID: PMC4068152
- DOI: 10.1016/j.jcmg.2011.08.019
Correlation between arterial FDG uptake and biomarkers in peripheral artery disease
Abstract
Objectives: A prospective, multicenter (18)fluorine-fluorodeoxyglucose ((18)F-FDG) positron emission tomography (PET)/computed tomography (CT) imaging study was performed to estimate the correlations among arterial FDG uptake and atherosclerotic plaque biomarkers in patients with peripheral artery disease.
Background: Inflammation within atherosclerotic plaques is associated with instability of the plaque and future cardiovascular events. Previous studies have shown that (18)F-FDG-PET/CT is able to quantify inflammation within carotid artery atherosclerotic plaques, but no studies to date have investigated this correlation in peripheral arteries with immunohistochemical confirmation.
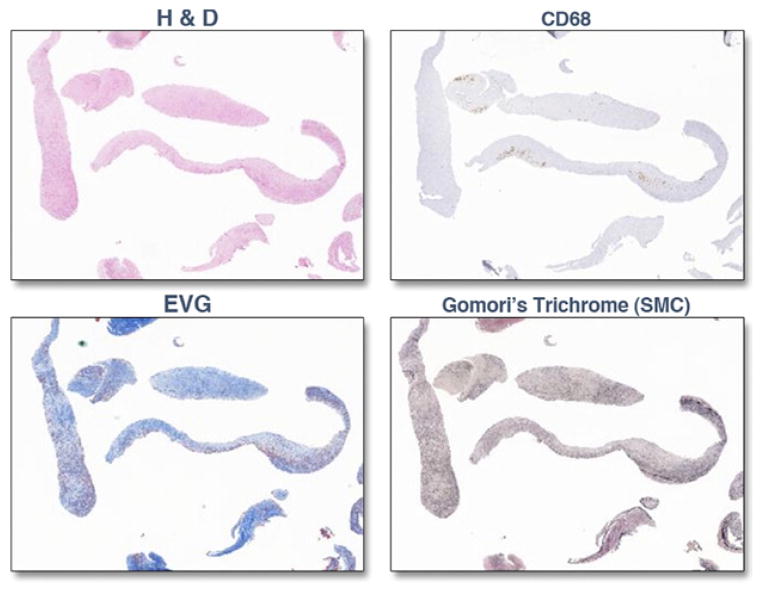
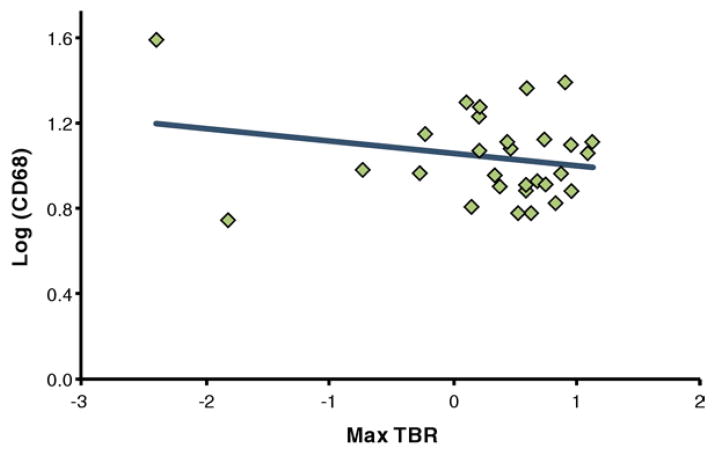
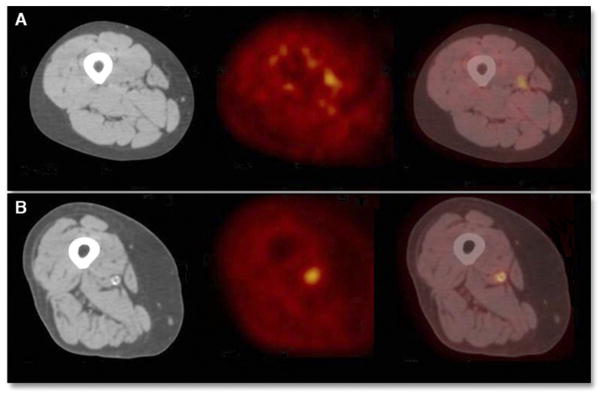
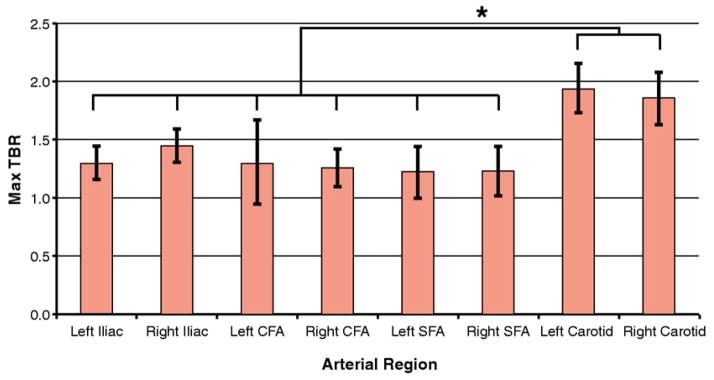
Methods: Thirty patients across 5 study sites underwent (18)F-FDG-PET/CT imaging before SilverHawk atherectomy (FoxHollow Technologies, Redwood City, California) for symptomatic common or superficial femoral arterial disease. Vascular FDG uptake (expressed as target-to-background ratio) was measured in the carotid arteries and aorta and femoral arteries, including the region of atherectomy. Immunohistochemistry was performed on the excised atherosclerotic plaque extracts, and cluster of differentiation 68 (CD68) level as a measure of macrophage content was determined. Correlations between target-to-background ratio of excised lesions, as well as entire arterial regions, and CD68 levels were determined. Imaging was performed during the 2 weeks before surgery in all cases.
Results: Twenty-one patients had adequate-quality (18)F-FDG-PET/CT peripheral artery images, and 34 plaque specimens were obtained. No significant correlation between lesion target-to-background ratio and CD68 level was observed.
Conclusions: There were no significant correlations between CD68 level (as a measure of macrophage content) and FDG uptake in the peripheral arteries in this multicenter study. Differences in lesion extraction technique, lesion size, the degree of inflammation, and imaging coregistration techniques may have been responsible for the failure to observe the strong correlations with vascular FDG uptake observed in previous studies of the carotid artery and in several animal models of atherosclerosis.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Libby P, Aikawa M. Inflammation in atherosclerosis. Nature. 2002;420:868–74. - PubMed
-
- Rudd JH, Myers KS, Sanz J, Fayad ZA. Multimodality imaging of atherosclerosis (magnetic resonance imaging/computed tomography/positron emission tomography-computed tomography) Top Magn Reson Imaging. 2007;18:379–88. - PubMed
-
- Rudd JH, Warburton EA, Fryer TD, et al. Imaging atherosclerotic plaque inflammation with [18F]-fluorodeoxyglucose positron emission tomography. Circulation. 2002;105:2708–11. - PubMed
-
- Davies JR, Rudd JH, Fryer TD, et al. Identification of culprit lesions after transient ischemic attack by combined 18F fluorodeoxyglucose positron-emission tomography and high-resolution magnetic resonance imaging. Stroke. 2005;36:2642–7. - PubMed
-
- Dunphy MP, Freiman A, Larson SM, Strauss HW. Association of vascular 18F-FDG uptake with vascular calcification. J Nucl Med. 2005;46:1278– 84. - PubMed
