

Diagnostic and prognostic stratification in the emergency department using urinary biomarkers of nephron damage: a multicenter prospective cohort study
- PMID: 22240130
- PMCID: PMC3487165
- DOI: 10.1016/j.jacc.2011.10.854
Diagnostic and prognostic stratification in the emergency department using urinary biomarkers of nephron damage: a multicenter prospective cohort study
Abstract
Objectives: This study aimed to determine the diagnostic and prognostic value of urinary biomarkers of intrinsic acute kidney injury (AKI) when patients were triaged in the emergency department.
Background: Intrinsic AKI is associated with nephron injury and results in poor clinical outcomes. Several urinary biomarkers have been proposed to detect and measure intrinsic AKI.
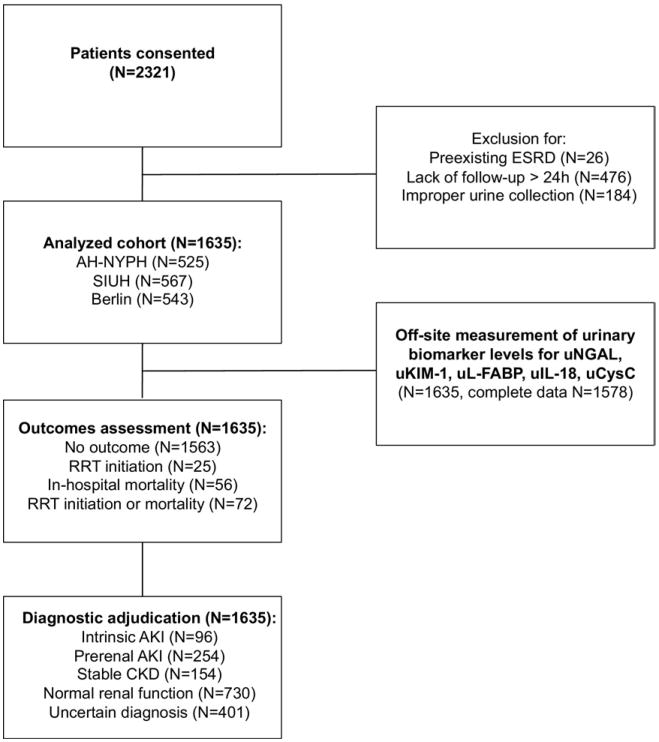
Methods: In a multicenter prospective cohort study, 5 urinary biomarkers (urinary neutrophil gelatinase-associated lipocalin, kidney injury molecule-1, urinary liver-type fatty acid binding protein, urinary interleukin-18, and cystatin C) were measured in 1,635 unselected emergency department patients at the time of hospital admission. We determined whether the biomarkers diagnosed intrinsic AKI and predicted adverse outcomes during hospitalization.
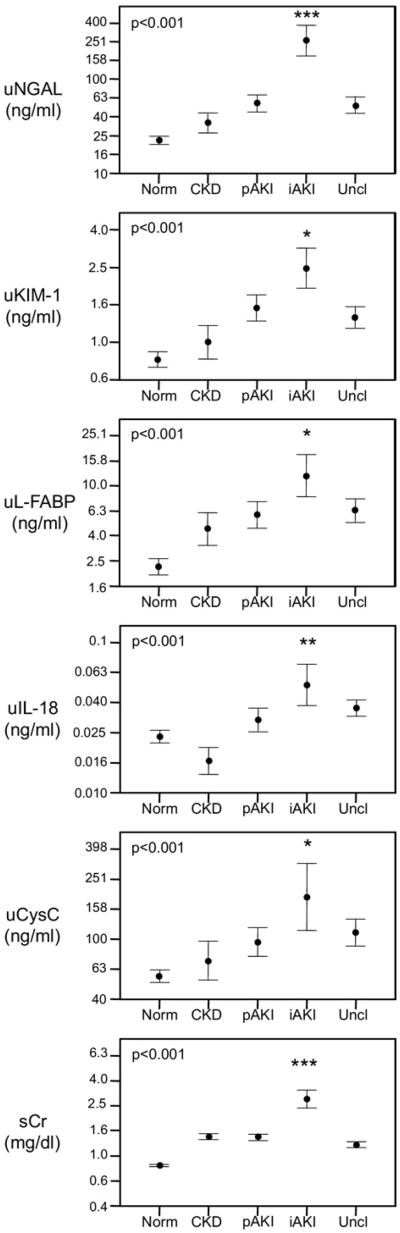
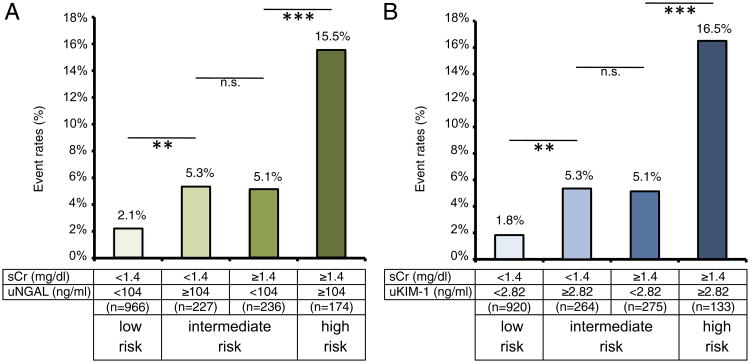
Results: All biomarkers were elevated in intrinsic AKI, but urinary neutrophil gelatinase-associated lipocalin was most useful (81% specificity, 68% sensitivity at a 104-ng/ml cutoff) and predictive of the severity and duration of AKI. Intrinsic AKI was strongly associated with adverse in-hospital outcomes. Urinary neutrophil gelatinase-associated lipocalin and urinary kidney injury molecule 1 predicted a composite outcome of dialysis initiation or death during hospitalization, and both improved the net risk classification compared with conventional assessments. These biomarkers also identified a substantial subpopulation with low serum creatinine at hospital admission, but who were at risk of adverse events.
Conclusions: Urinary biomarkers of nephron damage enable prospective diagnostic and prognostic stratification in the emergency department.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Acute kidney injury: urinary biomarkers of AKI for triage.Nat Rev Nephrol. 2012 Jan 31;8(3):131. doi: 10.1038/nrneph.2012.9. Nat Rev Nephrol. 2012. PMID: 22290541 No abstract available.
References
-
- Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16:3365–70. - PubMed
-
- Waikar SS, Curhan GC, Wald R, McCarthy EP, Chertow GM. Declining mortality in patients with acute renal failure, 1988 to 2002. J Am Soc Nephrol. 2006;17:1143–50. - PubMed
-
- Xue JL, Daniels F, Star RA, et al. Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992 to 2001. J Am Soc Nephrol. 2006;17:1135–42. - PubMed
-
- Liano F, Pascual J. Epidemiology of acute renal failure: a prospective, multicenter, community-based study. Madrid Acute Renal Failure Study Group. Kidney Int. 1996;50:811–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
