

Retinal detachment associated with optic disc colobomas and morning glory syndrome
- PMID: 22241012
- PMCID: PMC3325574
- DOI: 10.1038/eye.2011.354
Retinal detachment associated with optic disc colobomas and morning glory syndrome
Abstract
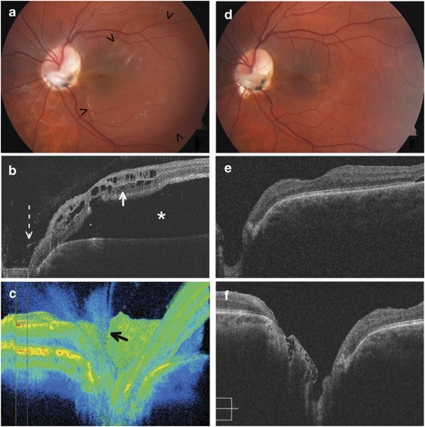
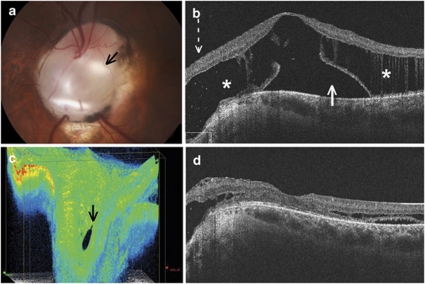
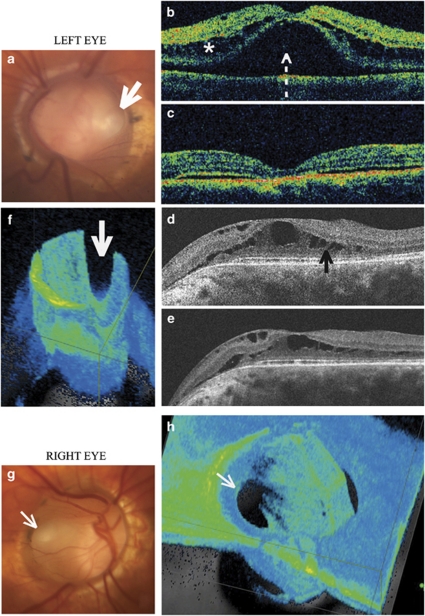
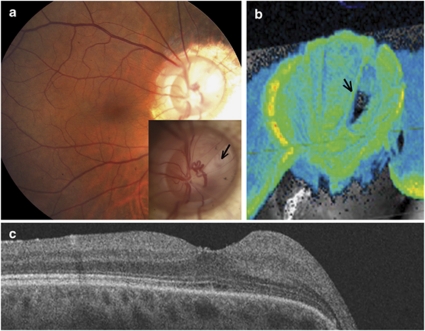
We report the diagnosis and treatment of patients with retinal detachment and/or retinoschisis associated with optic nerve coloboma or morning glory syndrome. A retrospective review of patients with optic nerve coloboma or morning glory syndrome with associated retinal detachment or retinoschisis was conducted. For five patients (six eyes), we report the clinical findings, spectral domain optical coherence tomography (OCT) imaging, intraoperative findings, and treatment outcomes. OCT scans demonstrate a bilaminar structure of maculopathy, consisting of inner schisis-like changes and outer layer retinal detachment. In most cases, a retinal break was demonstrated within the optic disc defect with three-dimensional OCT imaging. Glial tissue was sometimes observed within the anomalous defect. Vitrectomy and resection of the tractional tissue in these cases produced good anatomical and visual outcomes. Retinal detachment spontaneously resolved in cases where traction was not present. Traction may contribute to the pathogenesis of retinal detachment associated with colobomatous optic disc anomalies, either directly or by creating a secondary retinal break. OCT imaging assists with understanding the contributing factors to retinal detachment in individual cases of colobomatous optic disc anomalies and can thereby assist with determining the most effective approach to management.
Figures
Similar articles
-
Postoperative follow-up of a case of atypical morning glory syndrome associated with persistent fetal vasculature.BMC Ophthalmol. 2019 Jul 16;19(1):150. doi: 10.1186/s12886-019-1154-6. BMC Ophthalmol. 2019. PMID: 31311513 Free PMC article. Review.
-
Evaluation of congenital excavated optic disc anomalies with spectral-domain and swept-source optical coherence tomography.Graefes Arch Clin Exp Ophthalmol. 2014 Nov;252(11):1853-60. doi: 10.1007/s00417-014-2680-9. Epub 2014 Jun 7. Graefes Arch Clin Exp Ophthalmol. 2014. PMID: 24906342
-
Treatment of combined traction-rhegmatogenous retinal detachment in the morning glory syndrome.Retina. 1984 Fall-Winter;4(4):249-52. doi: 10.1097/00006982-198400440-00007. Retina. 1984. PMID: 6543402
-
Repair of retinal detachment associated with congenital excavated defects of the optic disc.Ophthalmic Surg. 1995 Jan-Feb;26(1):11-5. Ophthalmic Surg. 1995. PMID: 7746618
-
Congenital anomalies of the optic disc: insights from optical coherence tomography imaging.Curr Opin Ophthalmol. 2017 Nov;28(6):579-586. doi: 10.1097/ICU.0000000000000425. Curr Opin Ophthalmol. 2017. PMID: 28817389 Review.
Cited by
-
MORNING GLORY SYNDROME IN A NIGERIAN - A CASE REPORT.J West Afr Coll Surg. 2017 Jan-Mar;7(1):128-134. J West Afr Coll Surg. 2017. PMID: 29951459 Free PMC article.
-
Clinical and Echographic Features of Morning Glory Disc Anomaly in Children: A Retrospective Study of 249 Chinese Patients.Front Med (Lausanne). 2022 Jan 24;8:800623. doi: 10.3389/fmed.2021.800623. eCollection 2021. Front Med (Lausanne). 2022. PMID: 35141246 Free PMC article.
-
Evaluation of baseline optic disc pit and optic disc coloboma maculopathy features by spectral domain optical coherence tomography.Int J Retina Vitreous. 2023 Aug 7;9(1):46. doi: 10.1186/s40942-023-00484-7. Int J Retina Vitreous. 2023. PMID: 37550787 Free PMC article.
-
Postoperative follow-up of a case of atypical morning glory syndrome associated with persistent fetal vasculature.BMC Ophthalmol. 2019 Jul 16;19(1):150. doi: 10.1186/s12886-019-1154-6. BMC Ophthalmol. 2019. PMID: 31311513 Free PMC article. Review.
-
Management of Retinal Detachment Associated with Morning Glory Disc Syndrome.Case Rep Ophthalmol. 2021 May 25;12(2):457-463. doi: 10.1159/000516205. eCollection 2021 May-Aug. Case Rep Ophthalmol. 2021. PMID: 34177542 Free PMC article.
References
-
- Meirelles RL, Aggio FB, Costa RA, Farah ME. STRATUS optical coherence tomography in unilateral colobomatous excavation of the optic disc and secondary retinoschisis. Graefes Arch Clin Exp Ophthalmol. 2005;243:76–81. - PubMed
-
- Chang S, Haik BG, Ellsworth RM, St Louis L, Berrocal JA. Treatment of total retinal detachment in morning glory syndrome. Am J Ophthalmol. 1984;97:596–600. - PubMed
-
- Cennamo G, de Crecchio G, Iaccarino G, Forte R, Cennamo G. Evaluation of morning glory syndrome with spectral optical coherence tomography and echography. Ophthalmology. 2010;117:1269–1273. - PubMed
-
- Bartz-Schmidt KU, Heimann K. Pathogenesis of retinal detachment associated with morning glory disc. Int Ophthalmol. 1995;19:35–38. - PubMed
-
- Coll GE, Chang S, Flynn TE, Brown GC. Communication between the subretinal space and the vitreous cavity in the morning glory syndrome. Graefes Arch Clin Exp Ophthalmol. 1995;233:441–443. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
