

Dual-energy CT in the evaluation of intracerebral hemorrhage of unknown origin: differentiation between tumor bleeding and pure hemorrhage
- PMID: 22241388
- PMCID: PMC7968790
- DOI: 10.3174/ajnr.A2890
Dual-energy CT in the evaluation of intracerebral hemorrhage of unknown origin: differentiation between tumor bleeding and pure hemorrhage
Abstract
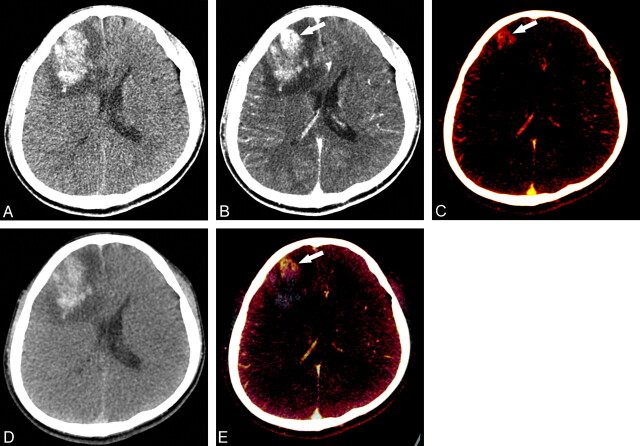
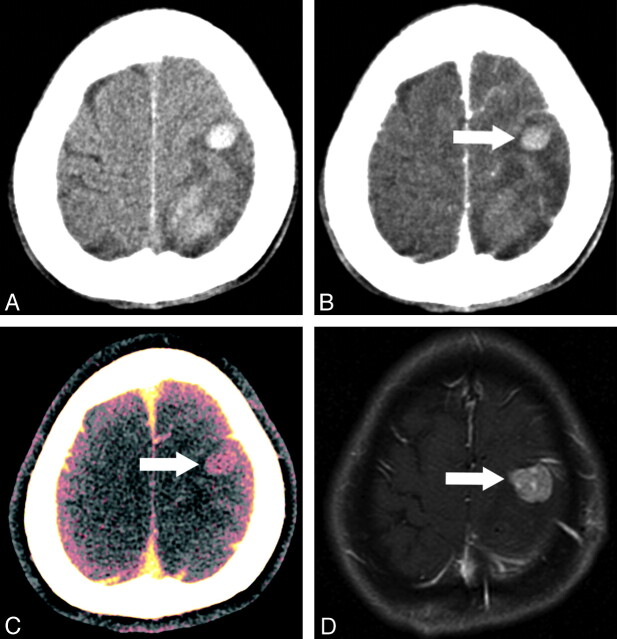
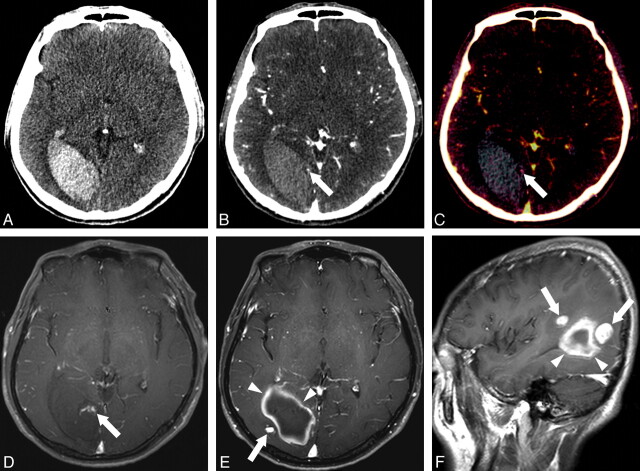
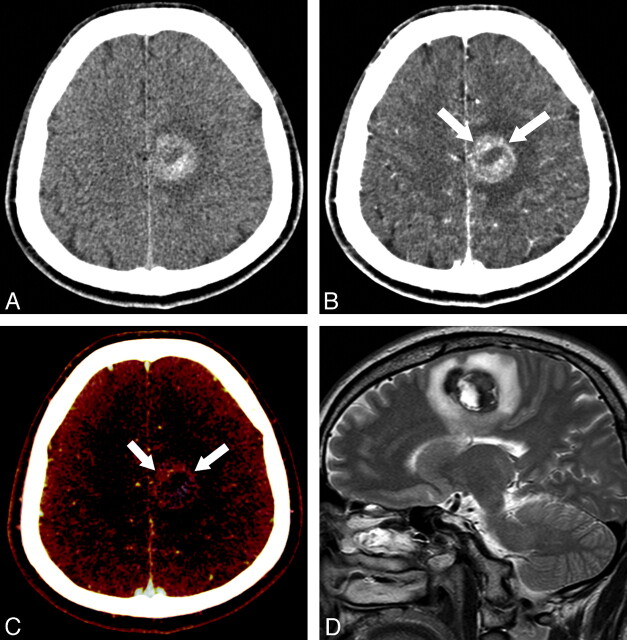
Background and purpose: Detection of underlying tumor in patients with unknown-origin acute ICH may be difficult because acute hematoma may mask enhancement of tumor on postcontrast CT. We intended to investigate the clinical utility of DECT in differentiating tumor bleeding from pure ICH.
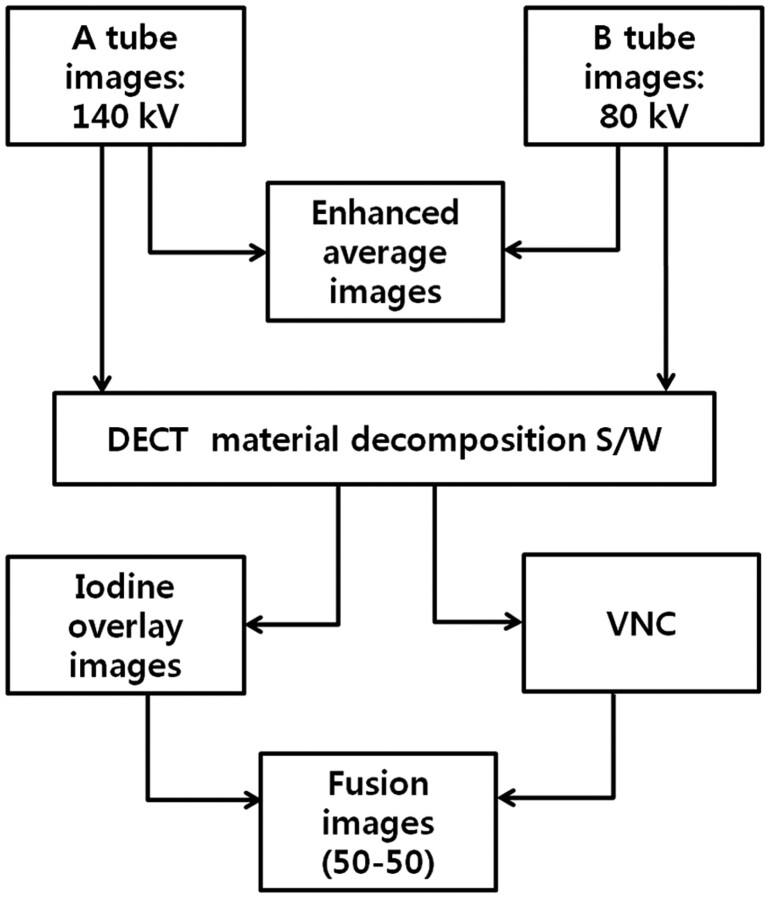
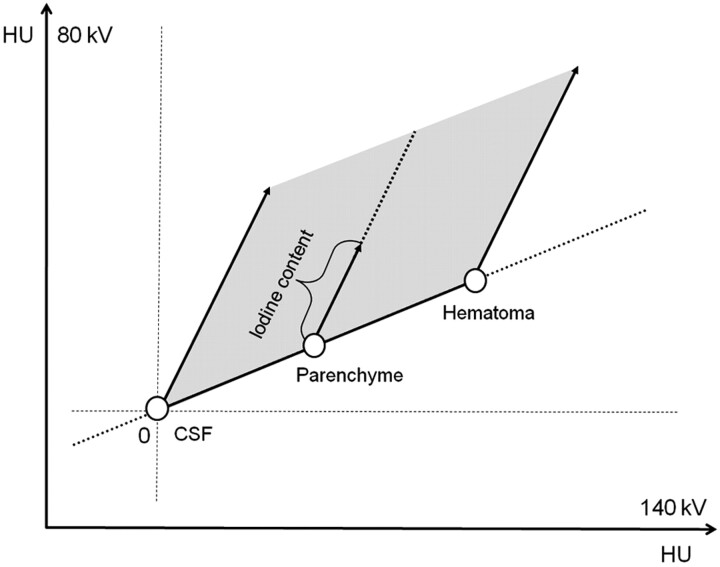
Materials and methods: Using a dual-source CT scanner, we obtained TNC single-energy and postcontrast DECT scans for 56 patients with unknown-origin spontaneous ICH. From the 2 sets of postcontrast DECT images obtained with different tube energy, EA (equivalent to conventional postcontrast CT), VNC, color-coded iodine overlay, fusion images of iodine overlay and VNC images were produced. The diagnostic performances of fusion, EA, and combined EA and TNC images for detecting underlying tumors were compared.
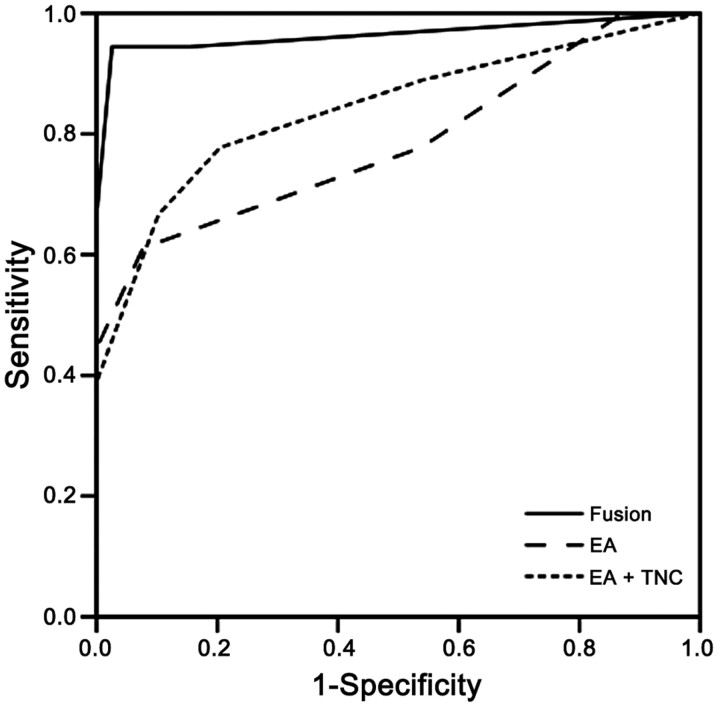
Results: Of the 56 patients, 17 had primary or metastatic tumors (18 lesions) and 39 had nontumorous ICH. The sensitivities of fusion, EA, and combined EA and TNC images for detecting brain tumors were 94.4%, 61.1%, and 66.7%, respectively, and their specificities were 97.4%, 92.3%, and 89.7%, respectively. The areas under the ROC curves were 0.964, 0.786, and 0.842, respectively. Overall, the diagnostic performance of fusion images was significantly superior to EA (P = .006) and combined EA and TNC (P = .011) images.
Conclusions: DECT may be useful in detecting underlying tumors in patients with unknown-origin ICH.
Figures
Similar articles
-
Virtual versus true non-contrast dual-energy CT imaging for the diagnosis of aortic intramural hematoma.Eur Radiol. 2019 Dec;29(12):6762-6771. doi: 10.1007/s00330-019-06322-5. Epub 2019 Jul 1. Eur Radiol. 2019. PMID: 31264015
-
Differentiation of hemorrhage from iodinated contrast in different intracranial compartments using dual-energy head CT.AJNR Am J Neuroradiol. 2012 Jun;33(6):1088-94. doi: 10.3174/ajnr.A2909. Epub 2012 Jan 19. AJNR Am J Neuroradiol. 2012. PMID: 22268092 Free PMC article. Clinical Trial.
-
Quantitative attenuation accuracy of virtual non-enhanced imaging compared to that of true non-enhanced imaging on dual-source dual-energy CT.Abdom Radiol (NY). 2020 Apr;45(4):1100-1109. doi: 10.1007/s00261-020-02415-8. Abdom Radiol (NY). 2020. PMID: 32052130
-
Dual-energy CT for differentiating acute intracranial hemorrhage from contrast staining or calcification: a meta-analysis.Neuroradiology. 2020 Dec;62(12):1617-1626. doi: 10.1007/s00234-020-02486-w. Epub 2020 Jul 4. Neuroradiology. 2020. PMID: 32621024
-
DECT in Detection of Vertebral Fracture-associated Bone Marrow Edema: A Systematic Review and Meta-Analysis with Emphasis on Technical and Imaging Interpretation Parameters.Radiology. 2021 Jul;300(1):110-119. doi: 10.1148/radiol.2021203624. Epub 2021 Apr 20. Radiology. 2021. PMID: 33876973
Cited by
-
Dual-energy CT: theoretical principles and clinical applications.Radiol Med. 2019 Dec;124(12):1281-1295. doi: 10.1007/s11547-019-01107-8. Epub 2019 Dec 2. Radiol Med. 2019. PMID: 31792703 Review.
-
Dual-energy CT for detection of contrast enhancement or leakage within high-density haematomas in patients with intracranial haemorrhage.Neuroradiology. 2014 Apr;56(4):291-5. doi: 10.1007/s00234-014-1333-3. Epub 2014 Feb 8. Neuroradiology. 2014. PMID: 24510167
-
Discrimination of Hemorrhage and Contrast Media in a Head Phantom on Photon-Counting Detector CT Data.AJNR Am J Neuroradiol. 2024 Feb 7;45(2):183-187. doi: 10.3174/ajnr.A8093. AJNR Am J Neuroradiol. 2024. PMID: 38164551 Free PMC article.
-
Prediction of infarction development after endovascular stroke therapy with dual-energy computed tomography.Eur Radiol. 2017 Mar;27(3):907-917. doi: 10.1007/s00330-016-4412-5. Epub 2016 Jun 2. Eur Radiol. 2017. PMID: 27255400 Free PMC article.
-
Dual energy CT: a step ahead in brain and spine imaging.Br J Radiol. 2020 May 1;93(1109):20190872. doi: 10.1259/bjr.20190872. Epub 2020 Jan 28. Br J Radiol. 2020. PMID: 31944834 Free PMC article.
References
-
- Broderick JP, Brott T, Tomsick T, et al. . The risk of subarachnoid and intracerebral hemorrhages in blacks as compared with whites. N Engl J Med 1992;326:733–36 - PubMed
-
- Furlan AJ, Whisnant JP, Elveback LR. The decreasing incidence of primary intracerebral hemorrhage: a population study. Ann Neurol 1979;5:367–73 - PubMed
-
- Qureshi AI, Tuhrim S, Broderick JP, et al. . Spontaneous intracerebral hemorrhage. N Engl J Med 2001;344:1450–60 - PubMed
-
- Fewel ME, Thompson BG, Hoff JT. Spontaneous intracerebral hemorrhage: a review. Neurosurg Focus 2003;15:E1 - PubMed
-
- Destian S, Sze G, Krol G, et al. . MR imaging of hemorrhagic intracranial neoplasms. AJR Am J Roentgenol 1989;152:137–44 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous