

Intracranial dural arteriovenous fistulas: classification, imaging findings, and treatment
- PMID: 22241393
- PMCID: PMC8013238
- DOI: 10.3174/ajnr.A2798
Intracranial dural arteriovenous fistulas: classification, imaging findings, and treatment
Abstract
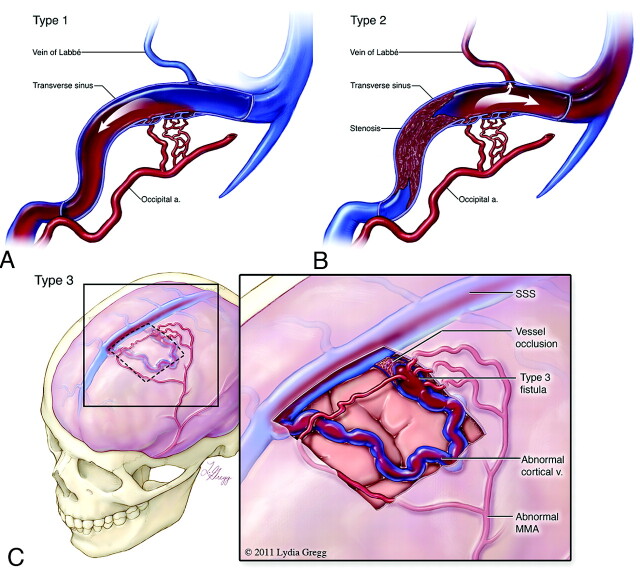
Intracranial DAVFs are pathologic dural-based shunts and account for 10%-15% of all intracranial arteriovenous malformations. These malformations derive their arterial supply primarily from meningeal vessels, and the venous drainage is either via dural venous sinuses or through the cortical veins. DAVFs have a reported association with dural sinus thrombosis, venous hypertension, previous craniotomy, and trauma, though many lesions are idiopathic. The diagnosis is dependent on a high level of clinical suspicion and high-resolution imaging. Cross-sectional imaging techniques by using CT and MR imaging aid in the diagnosis, but conventional angiography remains the most accurate method for complete characterization and classification of DAVFs. The pattern of venous drainage observed on dynamic vascular imaging determines the type of DAVF and correlates with the severity of symptoms and the risk of hemorrhage.
Figures


References
-
- Kirsch M, Liebig T, Kuhne D, et al. Endovascular management of dural arteriovenous fistulas of the transverse and sigmoid sinus in 150 patients. Neuroradiology 2009;51:477–83. Epub 2009 Apr 8 - PubMed
-
- Morita A, Meyer FB, Nichols DA, et al. Childhood dural arteriovenous fistulae of the posterior dural sinuses: three case reports and literature review. Neurosurgery 1995;37:1193–99, discussion 1199–1200 - PubMed
-
- Chung SJ, Kim JS, Kim JC, et al. Intracranial dural arteriovenous fistulas: analysis of 60 patients. Cerebrovasc Dis 2002;13:79–88 - PubMed
-
- Nabors MW, Azzam CJ, Albanna FJ, et al. Delayed postoperative dural arteriovenous malformations: report of two cases. J Neurosurg 1987;66:768–72 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical