

Estradiol promotes sudden cardiac death in transgenic long QT type 2 rabbits while progesterone is protective
- PMID: 22245795
- PMCID: PMC4397932
- DOI: 10.1016/j.hrthm.2012.01.009
Estradiol promotes sudden cardiac death in transgenic long QT type 2 rabbits while progesterone is protective
Abstract
Background: Postpubertal women with inherited long QT syndrome type 2 (LQT2) are at increased risk for polymorphic ventricular tachycardia (pVT) and sudden cardiac death (SCD), particularly during the postpartum period.
Objective: To investigate whether sex hormones directly modulate the arrhythmogenic risk in LQTS.
Methods: Prepubertal ovariectomized transgenic LQT2 rabbits were treated with estradiol (EST), progesterone (PROG), dihydrotestosterone (DHT), or placebo (OVX).
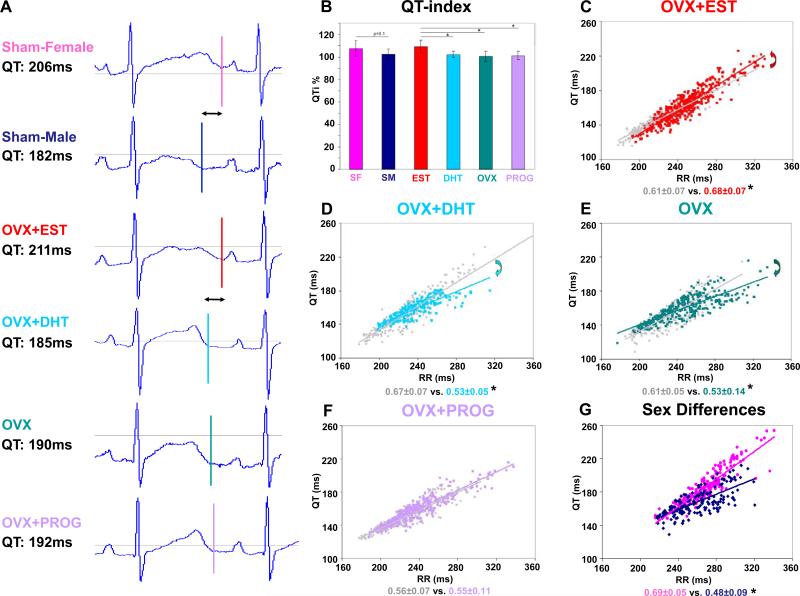
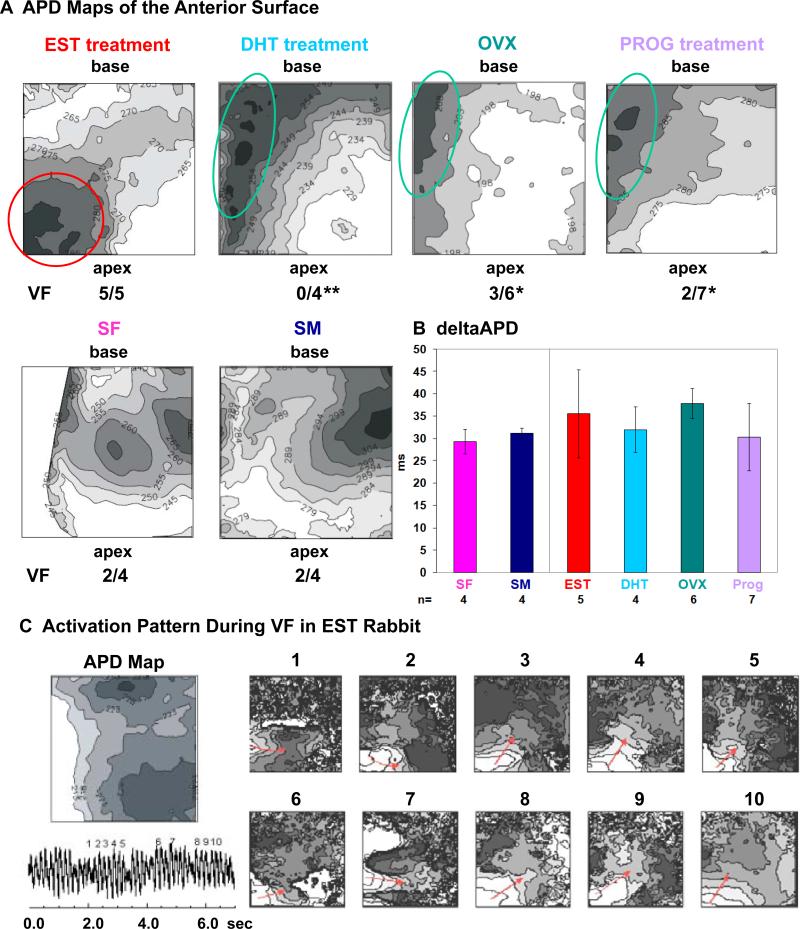
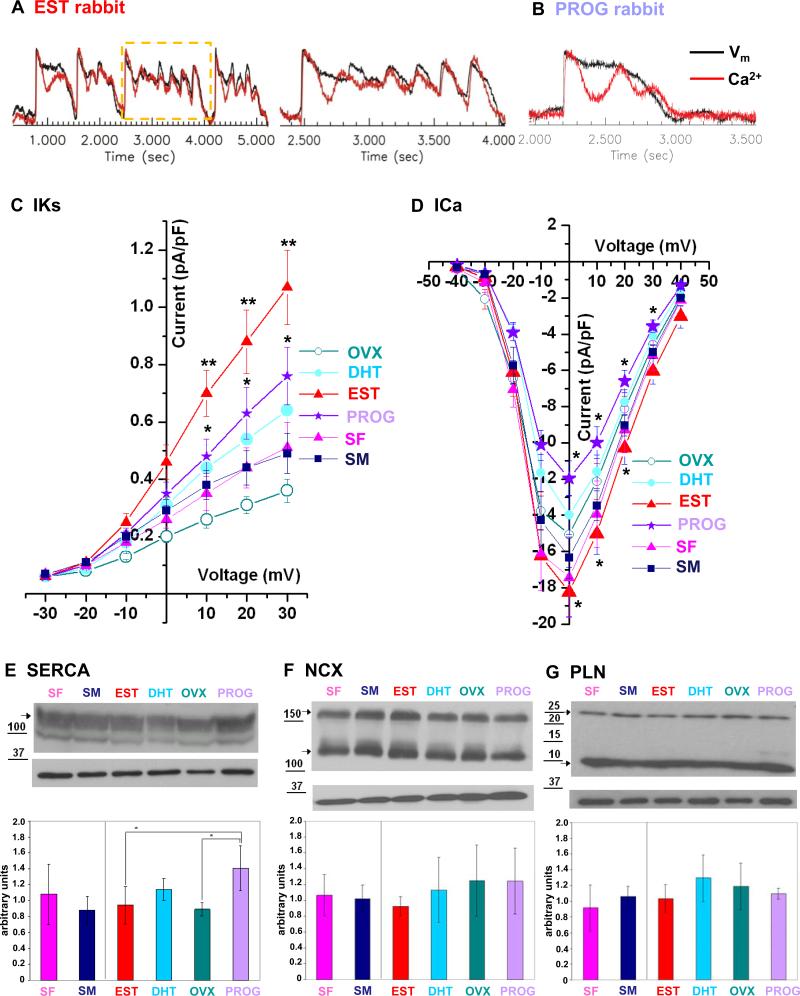
Results: During 8 weeks of treatment, major cardiac events-spontaneous pVT or SCD-occurred in 5 of the 7 EST rabbits and in 2 of the 9 OVX rabbits (P <.05); in contrast, no events occurred in 9 PROG rabbits and 6 DHT rabbits (P <.01 vs PROG; P <.05 vs DHT). Moreover, EST increased the incidence of pVT (P <.05 vs OVX), while PROG reduced premature ventricular contractions, bigeminy, couplets, triplets, and pVT (P <.01 vs OVX; P <.001 vs EST). In vivo electrocardiographic monitoring, in vivo electrophysiological studies, and ex vivo optical mapping studies revealed that EST promoted SCD by steepening the QT/RR slope (P <.05), by prolonging cardiac refractoriness (P <.05), and by altering the spatial pattern of action potential duration dispersion. Isoproterenol-induced Ca(2+) oscillations resulted in early afterdepolarizations in EST-treated hearts (4 of 4), while PROG prevented SCD by eliminating this early afterdepolarization formation in 4 of the 7 hearts (P = .058 vs EST; P <.05 vs OVX). Analyses of ion currents demonstrated that EST increased the density of I(Ca,L) as compared with OVX (P <.05) while PROG decreased it (P <.05).
Conclusion: This study reveals the proarrhythmic effect of EST and the antiarrhythmic effect of PROG in LQT2 in vivo, outlining a new potential antiarrhythmic therapy for LQTS.
Copyright © 2012 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Figures


Comment in
-
Sex hormones and ventricular tachyarrhythmias in LQTS: new insights regarding antiarrhythmic therapy.Heart Rhythm. 2012 May;9(5):833-4. doi: 10.1016/j.hrthm.2012.01.014. Epub 2012 Jan 20. Heart Rhythm. 2012. PMID: 22266129 No abstract available.
References
-
- Roden DM. Clinical practice. Long-QT syndrome. N Engl J Med. 2003;358:169–176. - PubMed
-
- Curran ME, Splawski I, Timothy KW, Vincent GM, Green ED, Keating MT. A molecular basis for cardiac arrhythmia: HERG mutations cause long-QT syndrome. Cell. 1995;80:795–803. - PubMed
-
- Sauer AJ, Moss AJ, McNitt S, et al. Long QT syndrome in adults. J Am Coll Cardiol. 2007;49:329–337. - PubMed
-
- Seth R, Moss AJ, McNitt S, et al. Long QT syndrome and pregnancy. J Am Coll Cardiol. 2007;49:1092–1098. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
