

Frequent detection of pancreatic lesions in asymptomatic high-risk individuals
- PMID: 22245846
- PMCID: PMC3321068
- DOI: 10.1053/j.gastro.2012.01.005
Frequent detection of pancreatic lesions in asymptomatic high-risk individuals
Abstract
Background & aims: The risk of pancreatic cancer is increased in patients with a strong family history of pancreatic cancer or a predisposing germline mutation. Screening can detect curable, noninvasive pancreatic neoplasms, but the optimal imaging approach is not known. We determined the baseline prevalence and characteristics of pancreatic abnormalities using 3 imaging tests to screen asymptomatic, high-risk individuals (HRIs).
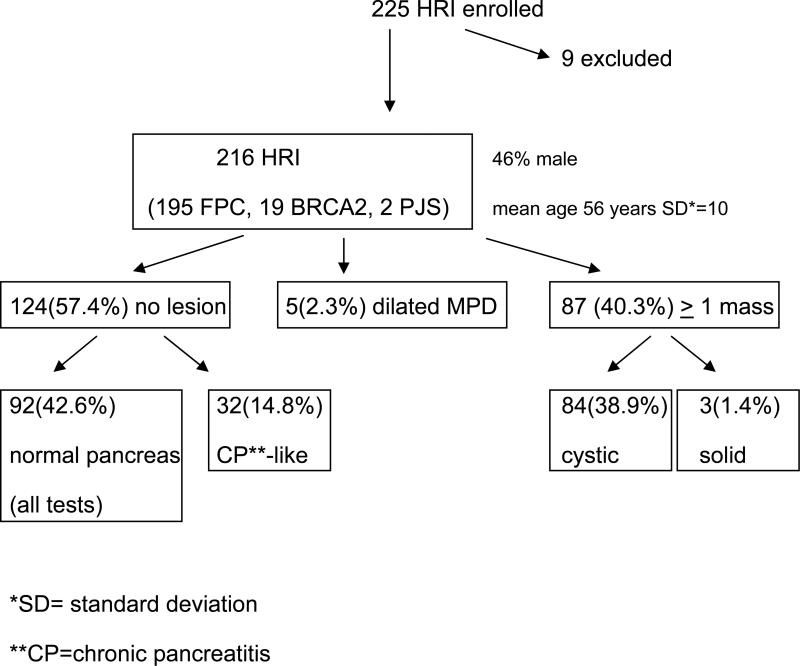
Methods: We screened 225 asymptomatic adult HRIs at 5 academic US medical centers once, using computed tomography (CT), magnetic resonance imaging (MRI), and endoscopic ultrasonography (EUS). We compared results in a blinded, independent fashion.
Results: Ninety-two of 216 HRIs (42%) were found to have at least 1 pancreatic mass (84 cystic, 3 solid) or a dilated pancreatic duct (n = 5) by any of the imaging modalities. Fifty-one of the 84 HRIs with a cyst (60.7%) had multiple lesions, typically small (mean, 0.55 cm; range, 2-39 mm), in multiple locations. The prevalence of pancreatic lesions increased with age; they were detected in 14% of subjects younger than 50 years old, 34% of subjects 50-59 years old, and 53% of subjects 60-69 years old (P < .0001). CT, MRI, and EUS detected a pancreatic abnormality in 11%, 33.3%, and 42.6% of the HRIs, respectively. Among these abnormalities, proven or suspected neoplasms were identified in 85 HRIs (82 intraductal papillary mucinous neoplasms and 3 pancreatic endocrine tumors). Three of 5 HRIs who underwent pancreatic resection had high-grade dysplasia in less than 3 cm intraductal papillary mucinous neoplasms and in multiple intraepithelial neoplasias.
Conclusions: Screening of asymptomatic HRIs frequently detects small pancreatic cysts, including curable, noninvasive high-grade neoplasms. EUS and MRI detect pancreatic lesions better than CT.
Copyright © 2012 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures


Comment in
-
Asymptomatic pancreatic lesions: new insights and clinical implications.World J Gastroenterol. 2012 Sep 7;18(33):4474-7. doi: 10.3748/wjg.v18.i33.4474. World J Gastroenterol. 2012. PMID: 22969218 Free PMC article.
References
-
- Giardiello FM, Brensinger JD, Tersmette AC, Goodman SN, Petersen GM, Booker SV, Cruz-Correa M, Offerhaus JA. Very high risk of cancer in familial Peutz-Jeghers syndrome. Gastroenterology. 2000;119:1447–53. - PubMed
-
- Lowenfels AB, Maisonneuve P, Cavallini G, Ammann RW, Lankisch PG, Andersen JR, Dimagno EP, Andren-Sandberg A, Domellof L. Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. N Engl J Med. 1993;328:1433–7. - PubMed
-
- Goldstein AM, Fraser MC, Struewing JP, Hussussian CJ, Ranade K, Zametkin DP, Fontaine LS, Organic SM, Dracopoli NC, Clark WH, et al. Increased risk of pancreatic cancer in melanoma-prone kindreds with p16INK4 mutations. N Engl J Med. 1995;333:970–4. - PubMed
-
- Thompson D, Easton DF. Cancer Incidence in BRCA1 mutation carriers. J Natl Cancer Inst. 2002;94:1358–65. - PubMed
-
- Hahn SA, Greenhalf B, Ellis I, Sina-Frey M, Rieder H, Korte B, Gerdes B, Kress R, Ziegler A, Raeburn JA, Campra D, Grutzmann R, Rehder H, Rothmund M, Schmiegel W, Neoptolemos JP, Bartsch DK. BRCA2 germline mutations in familial pancreatic carcinoma. J Natl Cancer Inst. 2003;95:214–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
