

The effectiveness of a new generation of computerized drug alerts in reducing the risk of injury from drug side effects: a cluster randomized trial
- PMID: 22246963
- PMCID: PMC3384117
- DOI: 10.1136/amiajnl-2011-000609
The effectiveness of a new generation of computerized drug alerts in reducing the risk of injury from drug side effects: a cluster randomized trial
Abstract
Context: Computerized drug alerts for psychotropic drugs are expected to reduce fall-related injuries in older adults. However, physicians over-ride most alerts because they believe the benefit of the drugs exceeds the risk.
Objective: To determine whether computerized prescribing decision support with patient-specific risk estimates would increase physician response to psychotropic drug alerts and reduce injury risk in older people.
Design: Cluster randomized controlled trial of 81 family physicians and 5628 of their patients aged 65 and older who were prescribed psychotropic medication.
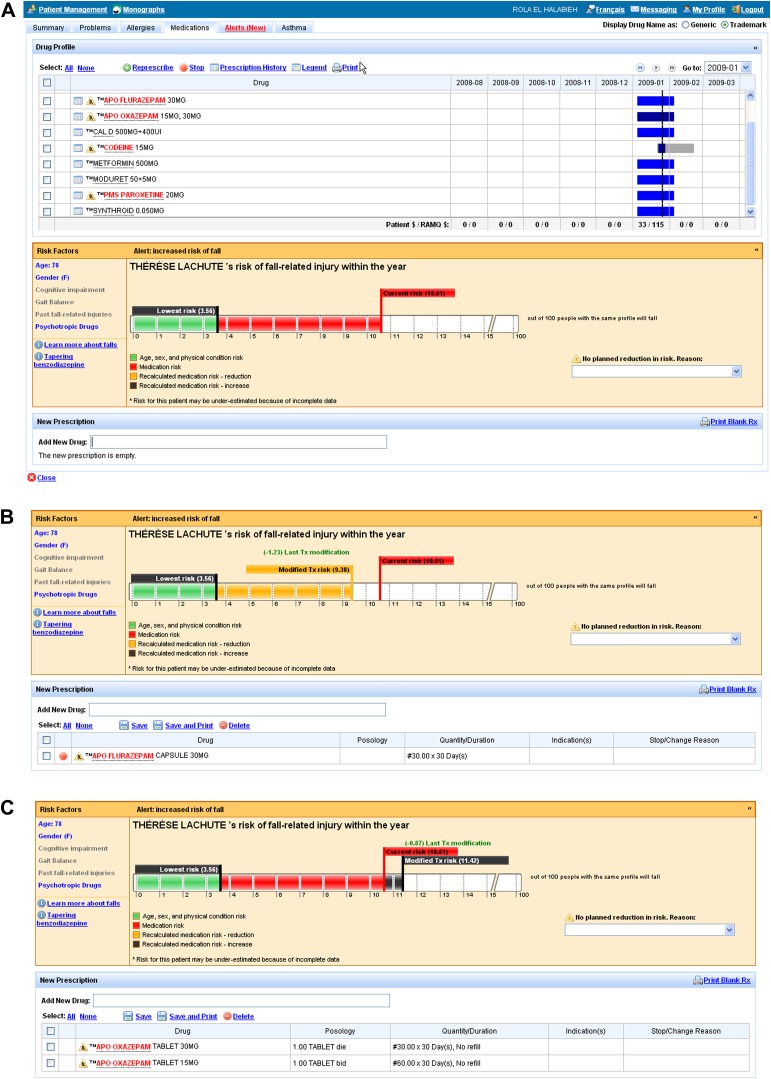
Intervention: Intervention physicians received information about patient-specific risk of injury computed at the time of each visit using statistical models of non-modifiable risk factors and psychotropic drug doses. Risk thermometers presented changes in absolute and relative risk with each change in drug treatment. Control physicians received commercial drug alerts.
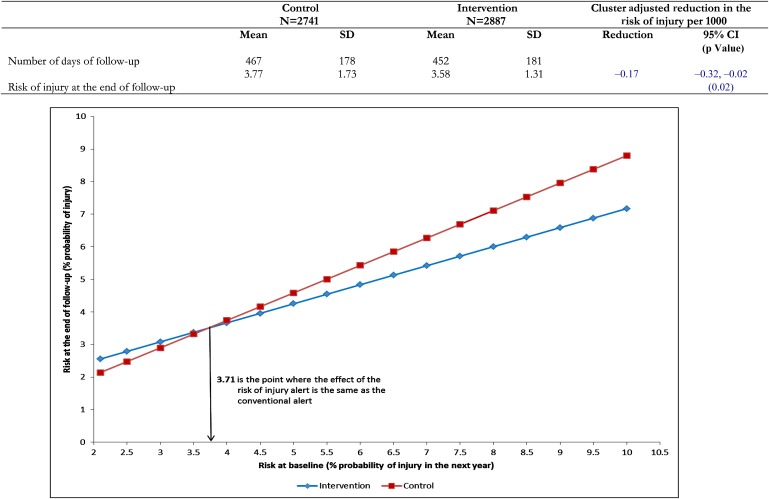
Main outcome measures: Injury risk at the end of follow-up based on psychotropic drug doses and non-modifiable risk factors. Electronic health records and provincial insurance administrative data were used to measure outcomes.
Results: Mean patient age was 75.2 years. Baseline risk of injury was 3.94 per 100 patients per year. Intermediate-acting benzodiazepines (56.2%) were the most common psychotropic drug. Intervention physicians reviewed therapy in 83.3% of visits and modified therapy in 24.6%. The intervention reduced the risk of injury by 1.7 injuries per 1000 patients (95% CI 0.2/1000 to 3.2/1000; p=0.02). The effect of the intervention was greater for patients with higher baseline risks of injury (p<0.03).
Conclusion: Patient-specific risk estimates provide an effective method of reducing the risk of injury for high-risk older people.
Trial registration number: clinicaltrials.gov Identifier: NCT00818285.
Conflict of interest statement
Figures


References
-
- Jemal A, Ward E, Hao Y, et al. Trends in the leading causes of death in the United States, 1970-2002. JAMA 2005;294:1255–9 - PubMed
-
- Centers for Disease Control and Prevention (CDC) Public health and aging: nonfatal injuries among older adults treated in hospital emergency departments–United States, 2001. MMWR Morb Mortal Wkly Rep 2003;52:1019–22 - PubMed
-
- Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clin Geriatr Med 2002;18:141–58 - PubMed
-
- Tinetti ME, Doucette J, Claus E, et al. Risk factors for serious injury during falls by older persons in the community. J Am Geriatr Soc 1995;43:1214–21 - PubMed
