

Attenuation of the pressor response to direct laryngoscopy and tracheal Intubation: oral clonidine vs. oral gabapentin premedication
- PMID: 22247722
- PMCID: PMC3252769
Attenuation of the pressor response to direct laryngoscopy and tracheal Intubation: oral clonidine vs. oral gabapentin premedication
Abstract
Background: We carried out this study to compare the efficacy of oral gabapentin and clonidine premedication for controlling the pressor responses to laryngoscopy and tracheal intubation.
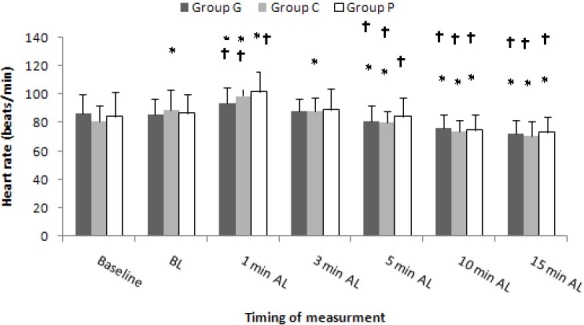
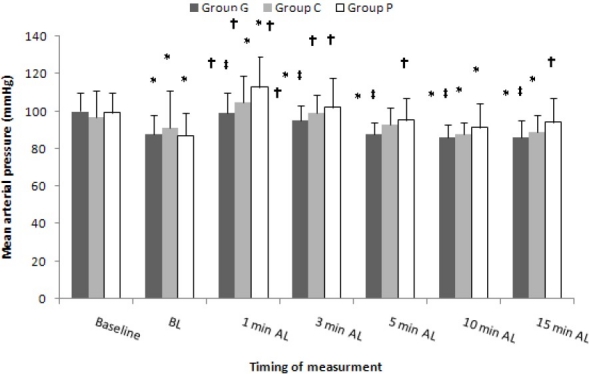
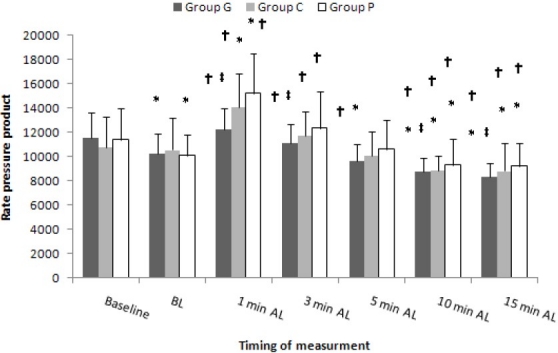
Methods: In this double-blind clinical trial, ninety-six patients were randomly allocated to one of three groups according to the agents to be used before the induction of anaesthesia: Group P (n = 32) received oral placebo, Group G (n = 32) received 800 mg of gabapentin, and Group C (n = 32) received 0.3 mg of clonidine 90 minutes prior to surgery. Systolic arterial pressure (SAP), diastolic arterial pressure (DAP), mean arterial pressure (MAP), heart rate (HR) and rate pressure product (RPP) were measured at baseline (3 min before induction), just before laryngoscopy, and postintubation (at 1, 3, 5, 10 and 15 min after starting laryngoscopy). Statistical analysis of data was done with repeated measure ANOVA and chi-square test.
Results: HR and RPP significantly decreased in Group G and Group C at 5, 10, and 15 minutes after tracheal intubation compared with those just before laryngoscopy (p < 0.05). No significant difference was noted between Group G and Group C considering these variables. SAP, DAP, MAP and RPP at 1, 3, 5, 10, and 15 minutes after intubation were significantly lower in Group G compared with Group P (p < 0.05). There was no significant difference between Group C and Group P in this regard.
Conclusions: The present study demonstrated that premedication with oral gabapentin 800 mg or clonidine 0.3 mg similarly blunted the hyperdynamic response after laryngoscopy and intubation.
Keywords: Premedication; intubation; laryngoscopy; oral clonidine; oral gabapentin; pressor response.
Conflict of interest statement
Figures
References
-
- Iannuzzi E, Iannuzzi M, Cirillo V, Viola G, Parisi R, Cerulli A, et al. Peri-intubation cardiovascular response during low dose remifentanil or sufentanil administration in association with propofol TCI.A double blind comparison. Minerva Anestesiol. 2004;70(3):109–15. - PubMed
-
- Russell WJ, Morris RG, Frewin DB, Drew SE. Changes in plasma catecholamine concentrations during endotracheal intubation. Br J Anaesth. 1981;53(8):837–9. - PubMed
-
- Edwards ND, Alford AM, Dobson PM, Peacock JE, Reilly CS. Myocardial ischaemia during tracheal intubation and extubation. Br J Anaesth. 1994;73(4):537–9. - PubMed
-
- Fox EJ, Sklar GS, Hill CH, Villanueva R, King BD. Complications related to the pressor response to endotracheal intubation. Anesthesiology. 1977;47(6):524–5. - PubMed
-
- Lunn JK, Stanley TH, Eisele J, Webster L, Woodward A. High dose fentanyl anesthesia for coronary artery surgery: plasma fentanyl concentrations and influence of nitrous oxide on cardiovascular responses. Anesth Analg. 1979;58(5):390–5. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous