

Anti-proteinase 3 anti-neutrophil cytoplasm autoantibodies recapitulate systemic vasculitis in mice with a humanized immune system
- PMID: 22247758
- PMCID: PMC3256135
- DOI: 10.1371/journal.pone.0028626
Anti-proteinase 3 anti-neutrophil cytoplasm autoantibodies recapitulate systemic vasculitis in mice with a humanized immune system
Abstract
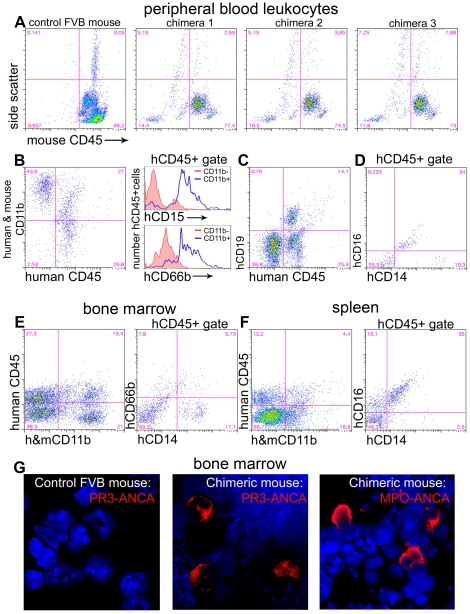
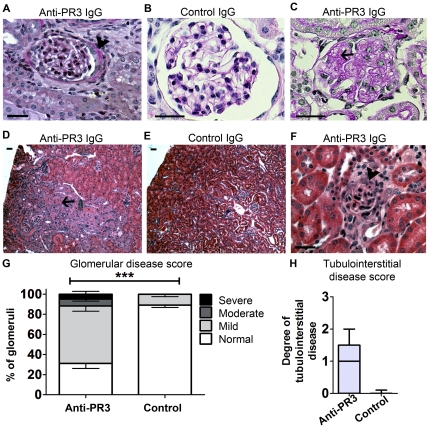
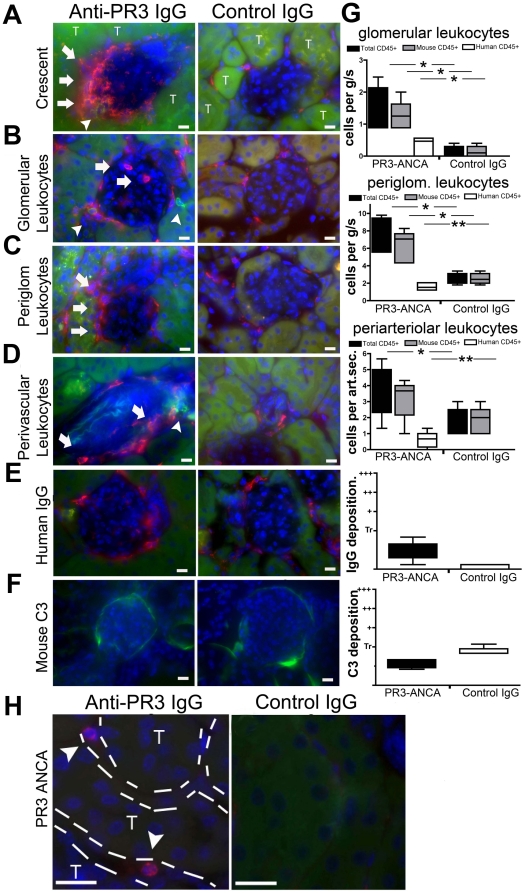
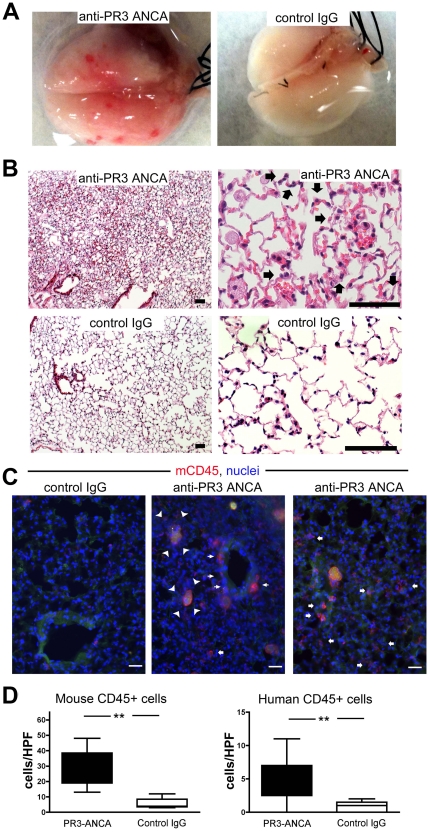
Evidence is lacking for direct pathogenicity of human anti-proteinase-3 (PR3) antibodies in development of systemic vasculitis and granulomatosis with polyangiitis (GPA, Wegener's granulomatosis). Progress in study of these antibodies in rodents has been hampered by lack of PR3 expression on murine neutrophils, and by different Fc-receptor affinities for IgG across species. Therefore, we tested whether human anti-PR3 antibodies can induce acute vasculitis in mice with a human immune system. Chimeric mice were generated by injecting human haematopoietic stem cells into irradiated NOD-scid-IL2Rγ⁻/⁻ mice. Matched chimera mice were treated with human IgG from patients with: anti-PR3 positive renal and lung vasculitis; patients with non-vasculitic renal disease; or healthy controls. Six-days later, 39% of anti-PR3 treated mice had haematuria, compared with none of controls. There was punctate bleeding on the surface of lungs of anti-PR3 treated animals, with histological evidence of vasculitis and haemorrhage. Anti-PR3 treated mice had mild pauci-immune proliferative glomerulonephritis, with infiltration of human and mouse leukocytes. In 3 mice (17%) more severe glomerular injury was present. There were no glomerular changes in controls. Human IgG from patients with anti-PR3 autoantibodies is therefore pathogenic. This model of anti-PR3 antibody-mediated vasculitis may be useful in dissecting mechanisms of microvascular injury.
Conflict of interest statement
Figures
References
-
- van der Woude FJ, Rasmussen N, Lobatto S, Wiik A, Permin H, et al. Autoantibodies against neutrophils and monocytes: tool for diagnosis and marker of disease activity in Wegener's granulomatosis. Lancet. 1985;1(8426):425–9. - PubMed
-
- Falk RJ, Jennette JC. Anti-neutrophil cytoplasmic autoantibodies with specificity for myeloperoxidase in patients with systemic vasculitis and idiopathic necrotizing and crescentic glomerulonephritis. N Engl J Med. 1988;318:1651–7. - PubMed
-
- Niles JL, McCluskey RT, Ahmad MF, Arnaout MA. Wegener's granulomatosis autoantigen is a novel neutrophil serine proteinase. Blood. 1989;74:1888–93. - PubMed
-
- Jennette JC, Hoidal JR, Falk RJ. Specificity of anti-neutrophil cytoplasmic autoantibodies for proteinase 3. Blood. 1990;75:2263–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
