

Chicago classification criteria of esophageal motility disorders defined in high resolution esophageal pressure topography
- PMID: 22248109
- PMCID: PMC3544361
- DOI: 10.1111/j.1365-2982.2011.01834.x
Chicago classification criteria of esophageal motility disorders defined in high resolution esophageal pressure topography
Abstract
Background: The Chicago Classification of esophageal motility was developed to facilitate the interpretation of clinical high resolution esophageal pressure topography (EPT) studies, concurrent with the widespread adoption of this technology into clinical practice. The Chicago Classification has been an evolutionary process, molded first by published evidence pertinent to the clinical interpretation of high resolution manometry (HRM) studies and secondarily by group experience when suitable evidence is lacking.
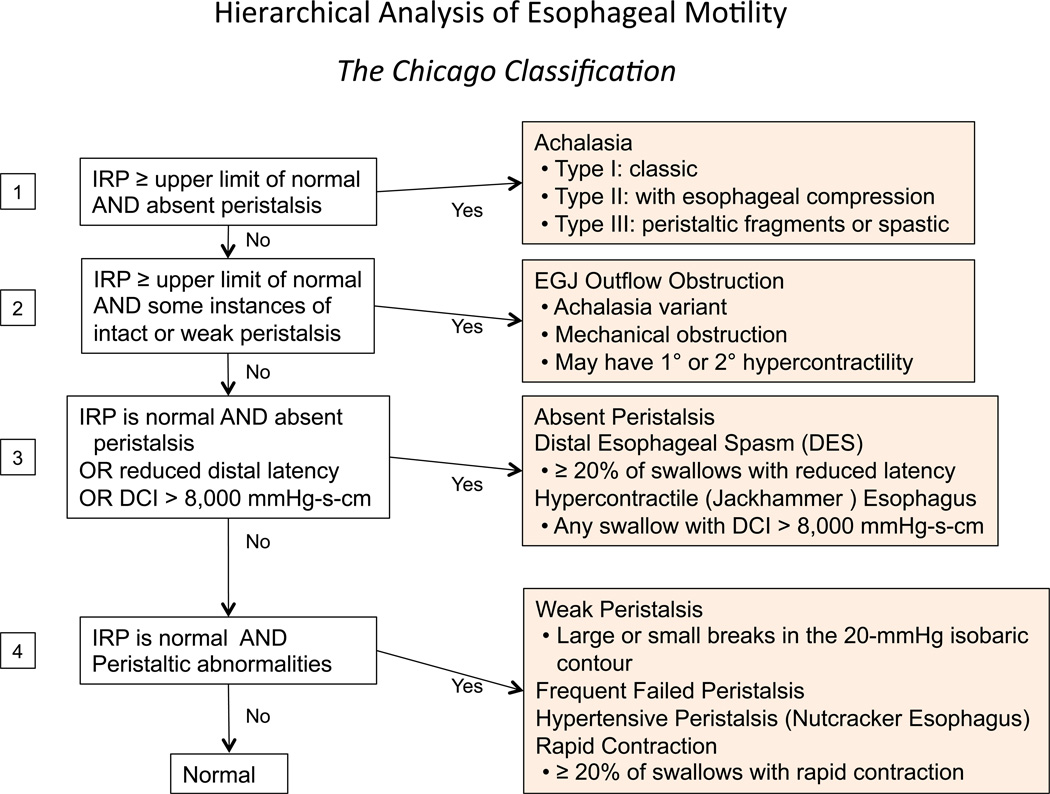
Purpose: This publication summarizes the state of our knowledge as of the most recent meeting of the International High Resolution Manometry Working Group in Ascona, Switzerland in April 2011. The prior iteration of the Chicago Classification was updated through a process of literature analysis and discussion. The major changes in this document from the prior iteration are largely attributable to research studies published since the prior iteration, in many cases research conducted in response to prior deliberations of the International High Resolution Manometry Working Group. The classification now includes criteria for subtyping achalasia, EGJ outflow obstruction, motility disorders not observed in normal subjects (Distal esophageal spasm, Hypercontractile esophagus, and Absent peristalsis), and statistically defined peristaltic abnormalities (Weak peristalsis, Frequent failed peristalsis, Rapid contractions with normal latency, and Hypertensive peristalsis). The Chicago Classification is an algorithmic scheme for diagnosis of esophageal motility disorders from clinical EPT studies. Moving forward, we anticipate continuing this process with increased emphasis placed on natural history studies and outcome data based on the classification.
© 2012 Blackwell Publishing Ltd.
Figures
References
-
- Clouse RE, Staiano A, Alrakawi A, Haroian L. Application of topographical methods to clinical esophageal manometry. Am J Gastroenterol. 2000;95:2720–2730. - PubMed
-
- Clouse RE, Staiano A. Topography of the esophageal peristaltic pressure wave. Am J Physiol. 1991;261:G677–G684. - PubMed
-
- Clouse RE, Staiano A. Topography of normal and high-amplitude esophageal peristalsis. Am J Physiol. 1993;265:G1098–G1107. - PubMed
-
- Staiano A, Clouse RE. The effects of cisapride on the topography of oesophageal peristalsis. Aliment Pharmacol Ther. 1996;10:875–882. - PubMed
-
- Clouse RE, Staiano A, Alrakawi A. Topographic analysis of esophageal double-peaked waves. Gastroenterology. 2000;118:469–476. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
