

Rituximab-induced direct inhibition of T-cell activation
- PMID: 22249775
- PMCID: PMC11029273
- DOI: 10.1007/s00262-011-1168-2
Rituximab-induced direct inhibition of T-cell activation
Abstract
Background: Rituximab, an anti-CD20 monoclonal antibody, is reported to increase the T-cell-dependent infection risk. The current study was designed to investigate whether rituximab interferes with T-cell activation.
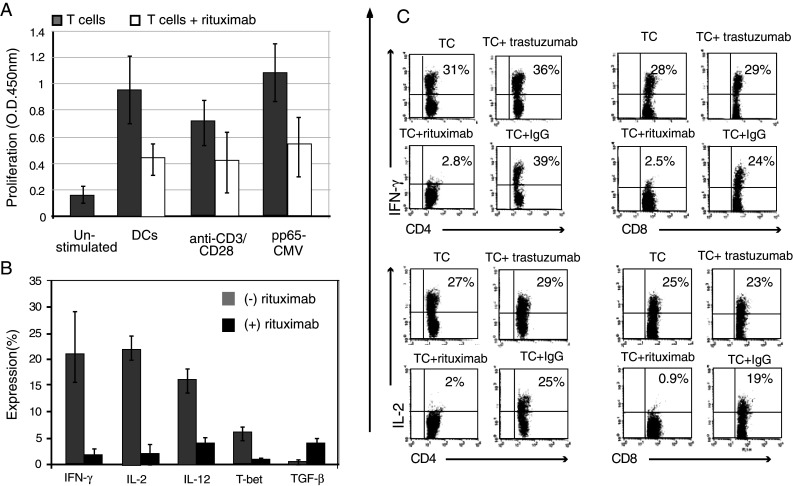
Patients and methods: Patients with non-Hodgkin lymphoma receiving 4-6 courses of 375 mg/m(2) rituximab underwent detailed assessment of T-cell activation pre- and post-rituximab. A similar analysis assessed the in vitro effect of rituximab on T-cell activation in response to allogeneic dendritic cells (allo-DCs) and other stimuli.
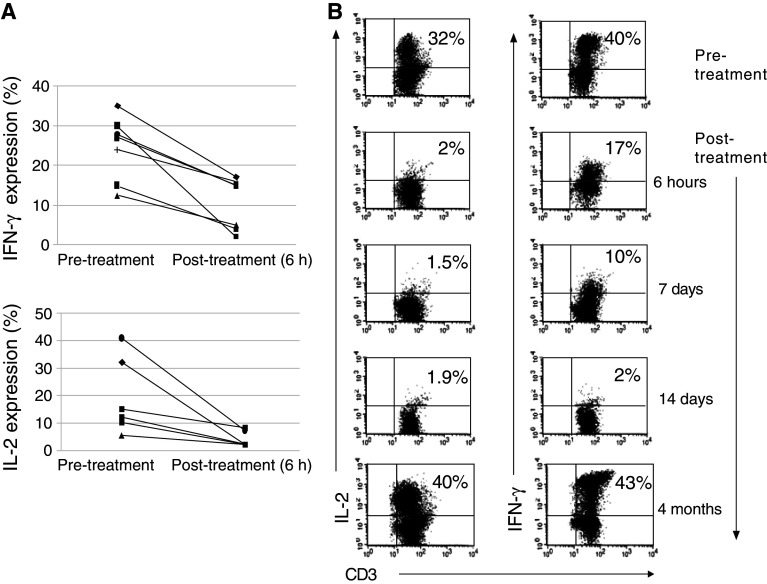
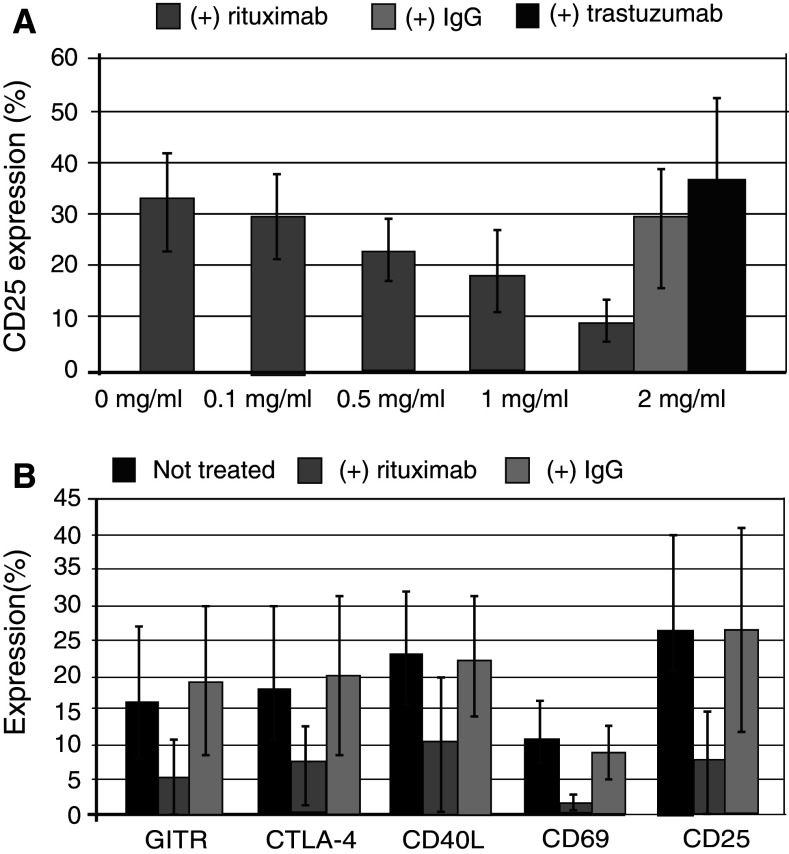
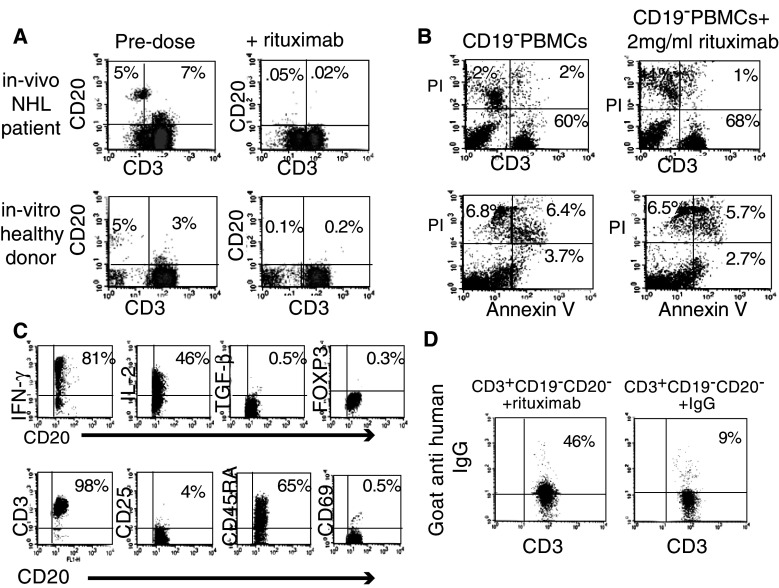
Results: Patients receiving rituximab exhibited a significant decline in IL-2 and IFN-γ levels in peripheral blood, most prominent after repeated rituximab courses. Evaluation at 3 months after rituximab therapy showed restoration of inflammatory cytokine production. Similarly, in vitro stimulation of peripheral blood mononuclear cells in the presence of rituximab resulted in a significant decrease in T-cell activation markers, inflammatory cytokine production and proliferative capacity. These effects were also observed using B-cell-depleted T cells (CD3(+)CD25(-)CD19(-)) and were accompanied with disappearance of CD3(+)CD20(dim) T-cell population.
Conclusion: Rituximab administration results in transient, dose-dependent T-cell inactivation. This effect is obtained even in B-cell absence and may increase the infection risk.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Rituximab: a review of its use in non-Hodgkin's lymphoma and chronic lymphocytic leukaemia.Drugs. 2003;63(8):803-43. doi: 10.2165/00003495-200363080-00005. Drugs. 2003. PMID: 12662126 Review.
-
A dose-escalation study of recombinant human interleukin-18 in combination with rituximab in patients with non-Hodgkin lymphoma.J Immunother. 2013 Jul-Aug;36(6):331-41. doi: 10.1097/CJI.0b013e31829d7e2e. J Immunother. 2013. PMID: 23799412 Free PMC article. Clinical Trial.
-
Bispecific T-Cell Engager (BiTE) Antibody Construct Blinatumomab for the Treatment of Patients With Relapsed/Refractory Non-Hodgkin Lymphoma: Final Results From a Phase I Study.J Clin Oncol. 2016 Apr 1;34(10):1104-11. doi: 10.1200/JCO.2014.59.1586. Epub 2016 Feb 16. J Clin Oncol. 2016. PMID: 26884582 Clinical Trial.
-
A single dose of rituximab does not deplete B cells in secondary lymphoid organs but alters phenotype and function.Am J Transplant. 2013 Jun;13(6):1503-11. doi: 10.1111/ajt.12220. Epub 2013 Apr 9. Am J Transplant. 2013. PMID: 23570303
-
Rituximab.Drugs. 1999 Jul;58(1):79-88; discussion 89-90. doi: 10.2165/00003495-199958010-00009. Drugs. 1999. PMID: 10439931 Review.
Cited by
-
Immunosuppressive Agents and Infectious Risk in Transplantation: Managing the "Net State of Immunosuppression".Clin Infect Dis. 2021 Oct 5;73(7):e1302-e1317. doi: 10.1093/cid/ciaa1189. Clin Infect Dis. 2021. PMID: 32803228 Free PMC article. Review.
-
Single fixed low-dose rituximab as induction therapy suppresses de novo donor-specific anti-HLA antibody production in ABO compatible living kidney transplant recipients.PLoS One. 2019 Oct 23;14(10):e0224203. doi: 10.1371/journal.pone.0224203. eCollection 2019. PLoS One. 2019. PMID: 31644555 Free PMC article.
-
Long-term outcome of childhood-onset complicated nephrotic syndrome after a multicenter, double-blind, randomized, placebo-controlled trial of rituximab.Pediatr Nephrol. 2017 Nov;32(11):2071-2078. doi: 10.1007/s00467-017-3718-0. Epub 2017 Jun 29. Pediatr Nephrol. 2017. PMID: 28664242 Clinical Trial.
-
What's new in neuromyelitis optica? A short review for the clinical neurologist.J Neurol. 2017 Nov;264(11):2330-2344. doi: 10.1007/s00415-017-8445-8. Epub 2017 Mar 13. J Neurol. 2017. PMID: 28289845 Review.
-
Herpes zoster development in living kidney transplant recipients receiving low-dose rituximab.Int J Urol. 2025 Jan;32(1):88-93. doi: 10.1111/iju.15600. Epub 2024 Oct 7. Int J Urol. 2025. PMID: 39373100 Free PMC article.
References
-
- McLaughlin P, Grillo-Lopez AJ, Link BK, Levy R, Czuczman MS, Williams ME, Heyman MR, Bence-Bruckler I, White CA, Cabanillas F, Jain V, Ho AD, Lister J, Wey K, Shen D, Dallaire BK. Rituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: half of patients respond to a four-dose treatment program. J Clin Oncol. 1998;16:2825–2833. - PubMed
-
- van Oers MH, Van Glabbeke M, Giurgea L, Klasa R, Marcus RE, Wolf M, Kimby E, van t Veer M, Vranovsky A, Holte H, Hagenbeek A. Rituximab maintenance treatment of relapsed/resistant follicular non-Hodgkin’s lymphoma: long-term outcome of the EORTC 20981 phase III randomized intergroup study. J Clin Oncol. 2010;28:2853–2858. doi: 10.1200/JCO.2009.26.5827. - DOI - PMC - PubMed
-
- Gisselbrecht C, Glass B, Mounier N, Singh Gill D, Linch DC, Trneny M, Bosly A, Ketterer N, Shpilberg O, Hagberg H, Ma D, Briere J, Moskowitz CH, Schmitz N. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28:4184–4190. doi: 10.1200/JCO.2010.28.1618. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
