

Pediatric analgesic clinical trial designs, measures, and extrapolation: report of an FDA scientific workshop
- PMID: 22250028
- PMCID: PMC9923552
- DOI: 10.1542/peds.2010-3591
Pediatric analgesic clinical trial designs, measures, and extrapolation: report of an FDA scientific workshop
Abstract
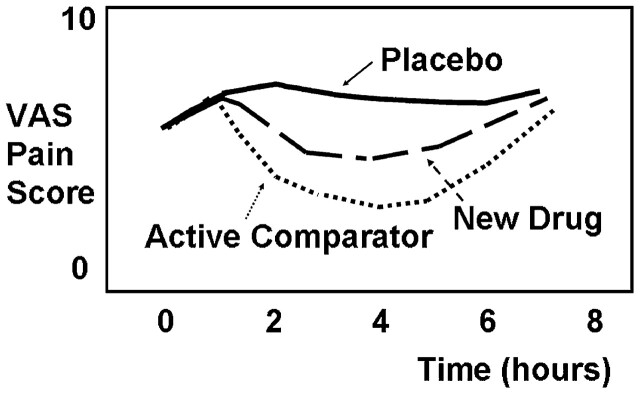
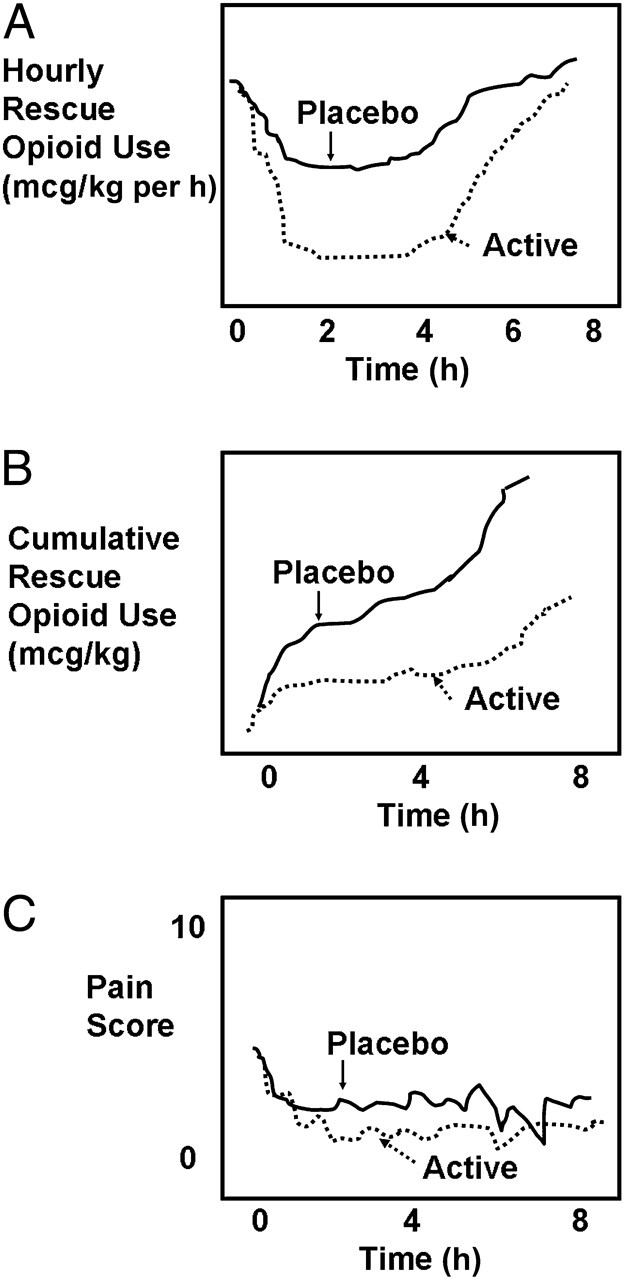
Analgesic trials pose unique scientific, ethical, and practical challenges in pediatrics. Participants in a scientific workshop sponsored by the US Food and Drug Administration developed consensus on aspects of pediatric analgesic clinical trial design. The standard parallel-placebo analgesic trial design commonly used for adults has ethical and practical difficulties in pediatrics, due to the likelihood of subjects experiencing pain for extended periods of time. Immediate-rescue designs using opioid-sparing, rather than pain scores, as a primary outcome measure have been successfully used in pediatric analgesic efficacy trials. These designs maintain some of the scientific benefits of blinding, with some ethical and practical advantages over traditional designs. Preferred outcome measures were recommended for each age group. Acute pain trials are feasible for children undergoing surgery. Pharmacodynamic responses to opioids, local anesthetics, acetaminophen, and nonsteroidal antiinflammatory drugs appear substantially mature by age 2 years. There is currently no clear evidence for analgesic efficacy of acetaminophen or nonsteroidal antiinflammatory drugs in neonates or infants younger than 3 months of age. Small sample designs, including cross-over trials and N of 1 trials, for particular pediatric chronic pain conditions and for studies of pain and irritability in pediatric palliative care should be considered. Pediatric analgesic trials can be improved by using innovative study designs and outcome measures specific for children. Multicenter consortia will help to facilitate adequately powered pediatric analgesic trials.
Conflict of interest statement
Figures
References
-
- Shaddy RE , Denne SC Committee on Drugs and Committee on Pediatric Research . Clinical report—guidelines for the ethical conduct of studies to evaluate drugs in pediatric populations. Pediatrics. 2010;125(4):850–860 - PubMed
-
- Weisman SJ , Bernstein B , Schechter NL . Consequences of inadequate analgesia during painful procedures in children. Arch Pediatr Adolesc Med. 1998;152(2):147–149 - PubMed
-
- 21 CFR. Section 50.53April, 2010
-
- E6 R. Guideline for Good Clinical Practice . In: I.C.H., ed, 1996. Available at: www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E.... Accessed January 9, 2012
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
