

Performance of the Canadian CT Head Rule and the New Orleans Criteria for predicting any traumatic intracranial injury on computed tomography in a United States Level I trauma center
- PMID: 22251188
- PMCID: PMC5637409
- DOI: 10.1111/j.1553-2712.2011.01247.x
Performance of the Canadian CT Head Rule and the New Orleans Criteria for predicting any traumatic intracranial injury on computed tomography in a United States Level I trauma center
Abstract
Objectives: This study compared the clinical performance of the Canadian CT Head Rule (CCHR) and the New Orleans Criteria (NOC) for detecting any traumatic intracranial lesion on computed tomography (CT) in patients with a Glasgow Coma Scale (GCS) score of 15. Also assessed were ability to detect patients with "clinically important" brain injury and patients requiring neurosurgical intervention. Additionally, the performance of the CCHR was assessed in a larger cohort of those presenting with GCS of 13 to 15.
Methods: This prospective cohort study was conducted in a U.S. Level I trauma center and enrolled a consecutive sample of mildly head-injured adults who presented to the emergency department (ED) with witnessed loss of consciousness, disorientation or amnesia, and GCS 13 to 15. The rules were compared in the group of patients with GCS 15. The primary outcome was prediction of "any traumatic intracranial injury" on CT. Secondary outcomes included "clinically important brain injury" on CT and need for neurosurgical intervention.
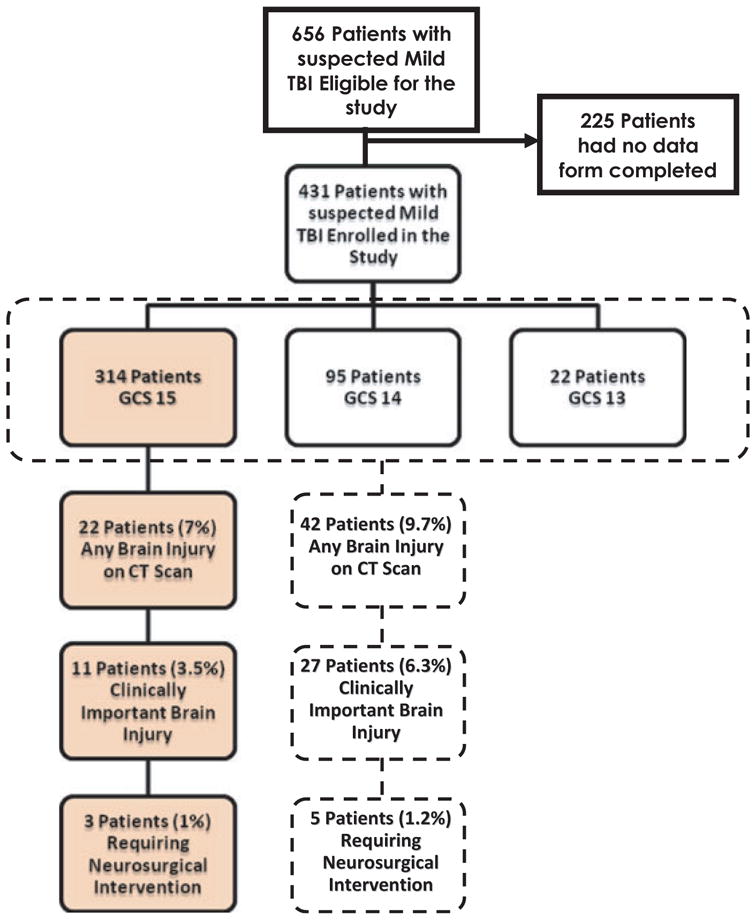
Results: Among the 431 enrolled patients, 314 patients (73%) had a GCS of 15, and 22 of the 314 (7%) had evidence of a traumatic intracranial lesion on CT. There were 11 of 314 (3.5%) who had "clinically important" brain injury, and 3 of 314 (1.0%) required neurosurgical intervention. The NOC and CCHR both had 100% sensitivity (95% confidence interval [CI] = 82% to 100%), but the CCHR was more specific for detecting any traumatic intracranial lesion on CT, with a specificity of 36.3% (95% CI = 31% to 42%) versus 10.2% (95% CI = 7% to 14%) for NOC. For "clinically important" brain lesions, the CCHR and the NOC had similar sensitivity (both 100%; 95% CI = 68% to 100%), but the specificity was 35% (95% CI = 30% to 41%) for CCHR and 9.9% (95% CI = 7% to 14%) for NOC. When the rules were compared for predicting need for neurosurgical intervention, the sensitivity was equivalent at 100% (95% CI = 31% to 100%) but the CCHR had a higher specificity at 80.7% (95% CI = 76% to 85%) versus 9.6% (95% CI = 7% to 14%) for NOC. Among all 431 patients with a GCS score 13 to 15, the CCHR had sensitivities of 100% (95% CI = 84% to 100%) for 27 patients with clinically important brain injury and 100% (95% CI = 46% to 100%) for five patients requiring neurosurgical intervention.
Conclusions: In a U.S. sample of mildly head-injured patients, the CCHR and the NOC had equivalently high sensitivities for detecting any traumatic intracranial lesion on CT, clinically important brain injury, and neurosurgical intervention, but the CCHR was more specific. A larger cohort will be needed to validate these findings.
© 2012 by the Society for Academic Emergency Medicine.
Conflict of interest statement
The authors have no relevant financial information or potential conflicts of interest to disclose.
Figures
References
-
- Faul M, Xu L, Wald MM, Coronado VG. Emergency Department Visits, Hospitalizations and Deaths 2002–2006. Atlanta (GA): Centers for Disease Control and Prevention; [Accessed Oct 23, 2011]. Traumatic Brain Injury in the United States. Available at: http://www.cdc.gov/traumaticbraininjury/pdf/blue_book.pdf.
-
- Centers for Disease Control and Prevention. Report to Congress on Mild Traumatic Brain Injury in the United States: Steps to Prevent a Serious Public Health Problem. Atlanta (GA): Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2003.
-
- af Geijerstam JL, Britton M. Mild head injury–mortality and complication rate: meta-analysis of findings in a systematic literature review. Acta Neurochir (Wien) 2003;145:843–50. - PubMed
-
- Jeret JS, Mandell M, Anziska B, et al. Clinical predictors of abnormality disclosed by computed tomography after mild head trauma. Neurosurgery. 1993;32:9–15. - PubMed
-
- Shackford SR, Wald SL, Ross SE, et al. The clinical utility of computed tomographic scanning and neurologic examination in the management of patients with minor head injuries. J Trauma. 1992;33:385–94. - PubMed
