

HPV DNA testing in population-based cervical screening (VUSA-Screen study): results and implications
- PMID: 22251922
- PMCID: PMC3305964
- DOI: 10.1038/bjc.2011.581
HPV DNA testing in population-based cervical screening (VUSA-Screen study): results and implications
Abstract
Background: Human papillomavirus (HPV) testing is more sensitive than cytology for detecting high-grade cervical intraepithelial neoplasia (CIN). We evaluated the performance of high-risk HPV (hrHPV) testing in routine screening.
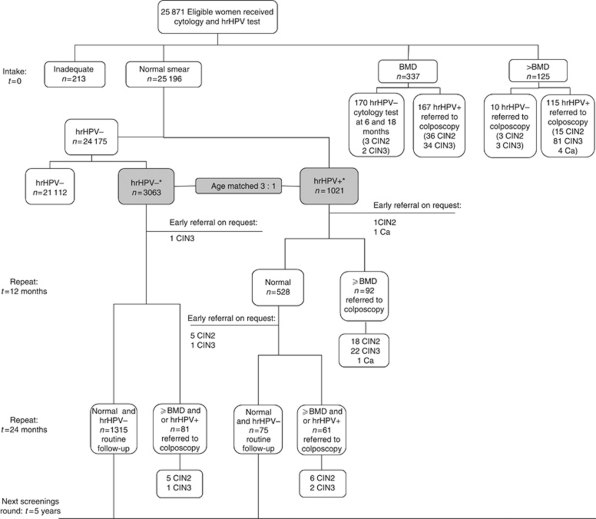
Methods: In all, 25,871 women (29-61) enrolled in our population-based cohort study were offered both cytology and hrHPV testing. High-risk HPV-positive women with normal cytology and an age-matched subcohort of hrHPV-negative women with normal cytology were invited for repeat testing after 1 and/or 2 years and were referred for colposcopy if they presented with abnormal cytology and/or a positive hrHPV test. The hrHPV-positive women with borderline or mild dyskaryosis (BMD) and all women with moderate dyskaryosis or worse (>BMD) were directly referred for colposcopy. Women with BMD and an hrHPV-negative test were advised to repeat cytology at 6 and 18 months and were referred for colposcopy if the repeat cytology test was abnormal. The main outcome measure was CIN grade 3 or worse (CIN3+). Results were adjusted for non-attendance at repeat testing.
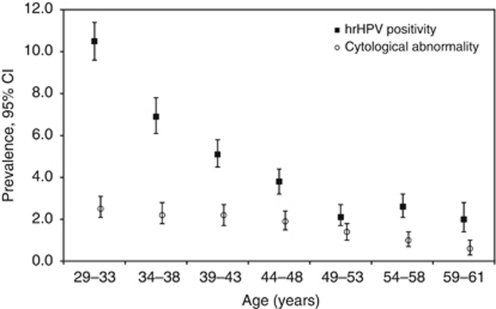
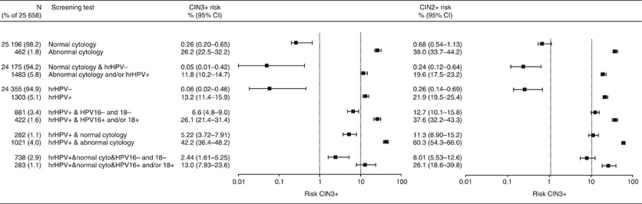
Results: The hrHPV-positive women with abnormal cytology had a CIN3+ risk of 42.2% (95% confidence interval (CI): 36.4-48.2), whereas the hrHPV-positive women with normal cytology had a much lower risk of 5.22% (95% CI: 3.72-7.91). In hrHPV-positive women with normal cytology, an additional cytology step after 1 year reduced the CIN3+ risk to only 1.6% (95% CI: 0.6-4.9) if the repeat test was normal. The CIN3+ risk in women with hrHPV-positive normal cytology was higher among women invited for the first time (29-33 years of age) (9.1%; 95% CI: 5.6-14.3) than among older women (3.0%; 95% CI: 1.5-5.5).
Conclusion: Primary hrHPV screening with cytology triage in women aged 30 years is an effective way to stratify women on CIN3+ risk and seems a feasible alternative to cytological screening. Repeat cytology after 1 year for hrHPV-positive women with normal cytology is however necessary before returning women to routine screening.
Figures
Comment in
-
Should human papillomavirus DNA testing be offered in combination with cytology or as a sole primary screening test in cervical cancer prevention?Future Oncol. 2012 Jul;8(7):783-6. doi: 10.2217/fon.12.62. Future Oncol. 2012. PMID: 22830399
Similar articles
-
Primary cervical cancer screening with HPV testing compared with liquid-based cytology: results of round 1 of a randomised controlled trial -- the HPV FOCAL Study.Br J Cancer. 2012 Dec 4;107(12):1917-24. doi: 10.1038/bjc.2012.489. Epub 2012 Nov 20. Br J Cancer. 2012. PMID: 23169286 Free PMC article. Clinical Trial.
-
Performance of carcinogenic human papillomavirus (HPV) testing and HPV16 or HPV18 genotyping for cervical cancer screening of women aged 25 years and older: a subanalysis of the ATHENA study.Lancet Oncol. 2011 Sep;12(9):880-90. doi: 10.1016/S1470-2045(11)70188-7. Epub 2011 Aug 22. Lancet Oncol. 2011. PMID: 21865084 Clinical Trial.
-
Age-specific evaluation of primary human papillomavirus screening vs conventional cytology in a randomized setting.J Natl Cancer Inst. 2009 Dec 2;101(23):1612-23. doi: 10.1093/jnci/djp367. Epub 2009 Nov 9. J Natl Cancer Inst. 2009. PMID: 19903804 Clinical Trial.
-
Evidence regarding human papillomavirus testing in secondary prevention of cervical cancer.Vaccine. 2012 Nov 20;30 Suppl 5:F88-99. doi: 10.1016/j.vaccine.2012.06.095. Vaccine. 2012. PMID: 23199969 Review.
-
Screening for Cervical Cancer With High-Risk Human Papillomavirus Testing: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Aug. Report No.: 17-05231-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Aug. Report No.: 17-05231-EF-1. PMID: 30256575 Free Books & Documents. Review.
Cited by
-
HPV-based Tests for Cervical Cancer Screening and Management of Cervical Disease.Curr Obstet Gynecol Rep. 2013 Jun 1;2(2):76-85. doi: 10.1007/s13669-013-0040-0. Curr Obstet Gynecol Rep. 2013. PMID: 23705102 Free PMC article.
-
Risk-stratification of HPV-positive women with low-grade cytology by FAM19A4/miR124-2 methylation and HPV genotyping.Br J Cancer. 2022 Feb;126(2):259-264. doi: 10.1038/s41416-021-01614-4. Epub 2021 Nov 6. Br J Cancer. 2022. PMID: 34743198 Free PMC article.
-
Human papillomavirus type-specific prevalence in the cervical cancer screening population of Czech women.PLoS One. 2013 Nov 12;8(11):e79156. doi: 10.1371/journal.pone.0079156. eCollection 2013. PLoS One. 2013. PMID: 24265750 Free PMC article.
-
Recent advances in understanding and preventing human papillomavirus-related disease.F1000Res. 2017 Mar 14;6:F1000 Faculty Rev-269. doi: 10.12688/f1000research.9701.1. eCollection 2017. F1000Res. 2017. PMID: 28357043 Free PMC article. Review.
-
Point-of-Care Digital Cytology With Artificial Intelligence for Cervical Cancer Screening in a Resource-Limited Setting.JAMA Netw Open. 2021 Mar 1;4(3):e211740. doi: 10.1001/jamanetworkopen.2021.1740. JAMA Netw Open. 2021. PMID: 33729503 Free PMC article.
References
-
- Anderson MC (1995) Premalignant and malignant squamous lesions of the cervix. In: Fox H, Wells M (eds). Obstetrical and Gynaecological Pathology , 4th edn. Churchill Livingstone: New York, pp 292–297
-
- Arbyn M, Raifu AO, Weiderpass E, Bray F, Anttila A (2009) Trends of cervical cancer mortality in the member states of the European Union. Eur J Cancer 45: 2640–2648 - PubMed
-
- Arbyn M, Sasieni P, Meijer CJ, Clavel C, Koliopoulos G, Dillner J (2006) Chapter 9: Clinical applications of HPV testing: a summary of meta-analyses. Vaccine 24(Suppl 3): S78–S89 - PubMed
-
- Bulk S, Bulkmans NW, Berkhof J, Rozendaal L, Boeke AJ, Verheijen RH, Snijders PJ, Meijer CJ (2007) Risk of high-grade cervical intra-epithelial neoplasia based on cytology and high-risk HPV testing at baseline and at 6-months. Int J Cancer 121: 361–367 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
