

Bridging antiplatelet therapy with cangrelor in patients undergoing cardiac surgery: a randomized controlled trial
- PMID: 22253393
- PMCID: PMC3774162
- DOI: 10.1001/jama.2011.2002
Bridging antiplatelet therapy with cangrelor in patients undergoing cardiac surgery: a randomized controlled trial
Abstract
Context: Thienopyridines are among the most widely prescribed medications, but their use can be complicated by the unanticipated need for surgery. Despite increased risk of thrombosis, guidelines recommend discontinuing thienopyridines 5 to 7 days prior to surgery to minimize bleeding.
Objective: To evaluate the use of cangrelor, an intravenous, reversible P2Y(12) platelet inhibitor for bridging thienopyridine-treated patients to coronary artery bypass grafting (CABG) surgery.
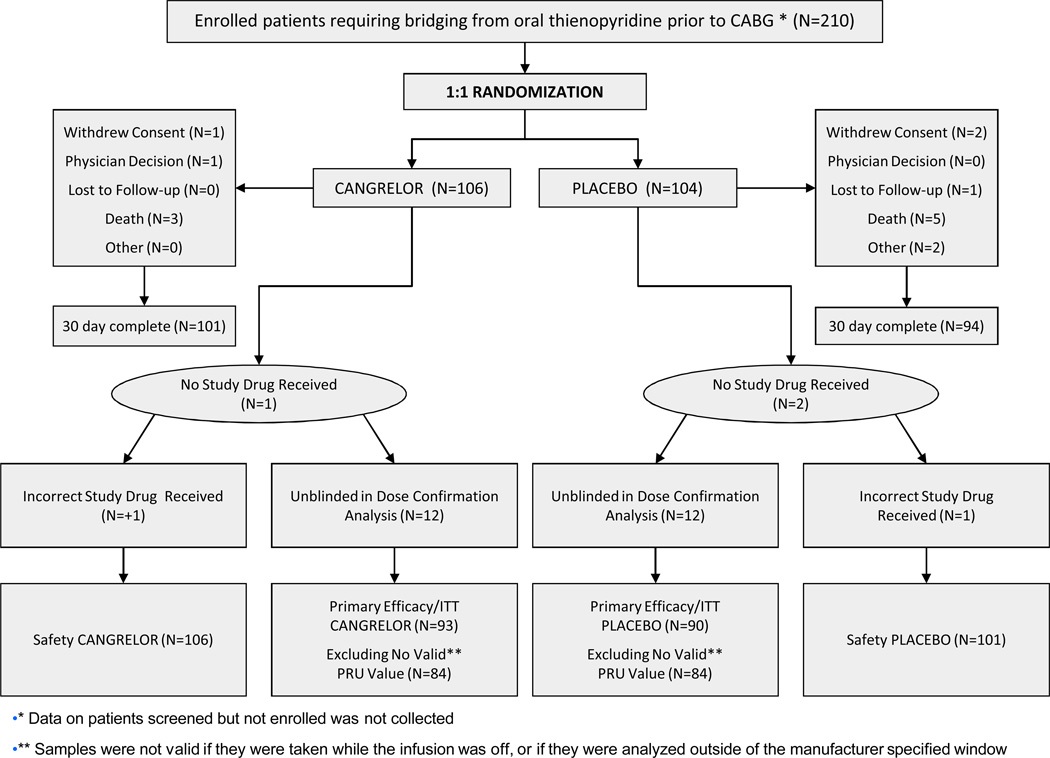
Design, setting, and patients: Prospective, randomized, double-blind, placebo-controlled, multicenter trial, involving 210 patients with an acute coronary syndrome (ACS) or treated with a coronary stent and receiving a thienopyridine awaiting CABG surgery to receive either cangrelor or placebo after an initial open-label, dose-finding phase (n = 11) conducted between January 2009 and April 2011. Interventions Thienopyridines were stopped and patients were administered cangrelor or placebo for at least 48 hours, which was discontinued 1 to 6 hours before CABG surgery.
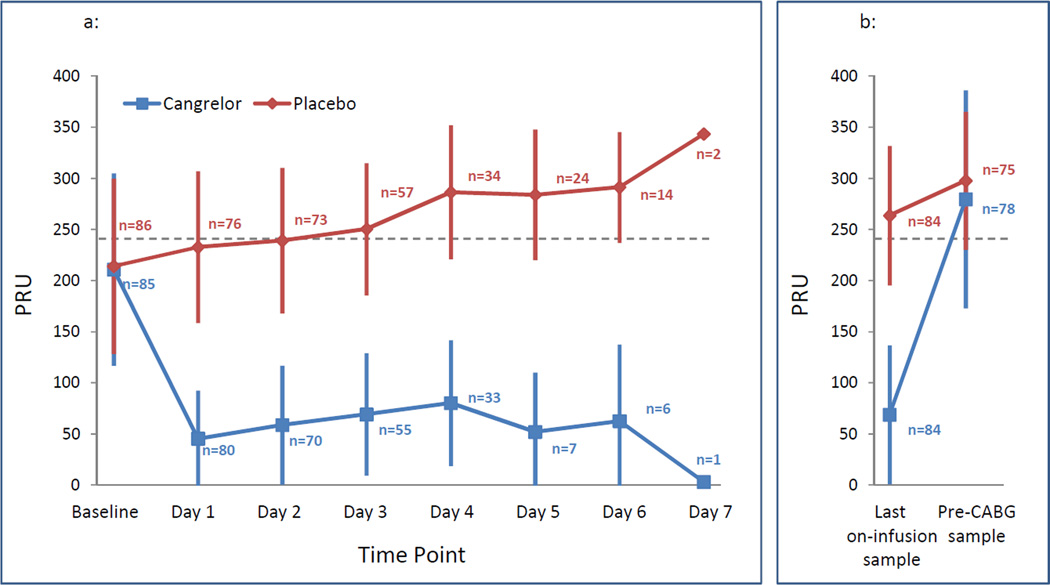
Main outcome measures: The primary efficacy end point was platelet reactivity (measured in P2Y(12) reaction units [PRUs]), assessed daily. The main safety end point was excessive CABG surgery-related bleeding.
Results: The dose of cangrelor determined in 10 patients in the open-label stage was 0.75 μg/kg per minute. In the randomized phase, a greater proportion of patients treated with cangrelor had low levels of platelet reactivity throughout the entire treatment period compared with placebo (primary end point, PRU <240; 98.8% (83 of 84) vs 19.0% (16 of 84); relative risk [RR], 5.2 [95% CI, 3.3-8.1] P < .001). Excessive CABG surgery-related bleeding occurred in 11.8% (12 of 102) vs 10.4% (10 of 96) in the cangrelor and placebo groups, respectively (RR, 1.1 [95% CI, 0.5-2.5] P = .763). There were no significant differences in major bleeding prior to CABG surgery, although minor bleeding episodes were numerically higher with cangrelor.
Conclusions: Among patients who discontinue thienopyridine therapy prior to cardiac surgery, the use of cangrelor compared with placebo resulted in a higher rate of maintenance of platelet inhibition.
Trial registration: clinicaltrials.gov Identifier: NCT00767507.
Figures
References
-
- Anderson JL, Adams CD, Antman EM, et al. WRITING GROUP MEMBERS; ACCF/AHA TASK FORCE MEMBERS. 2011 ACCF/AHA Focused Update Incorporated Into the ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011 May 10;123(18):e426–e579. - PubMed
-
- Kushner FG, Hand M, Smith SC, Jr., et al. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2009 Focused Updates: ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction (updating the 2004 Guideline and 2007 Focused Update) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (updating the 2005 Guideline and 2007 Focused Update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2009 Dec 1;120(22):2271–2306. - PubMed
-
- Wijns W, Kolh P, Danchin N, et al. European Association for Percutaneous Cardiovascular Interventions/ESC Committee for Practice Guidelines. Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J. 2010 Oct;31(20):2501–2555. - PubMed
-
- Hamm CW, Bassand JP, Agewall S, et al. ESC Committee for Practice Guidelines. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2011 Aug 26; [Epub ahead of print] - PubMed
-
- Ho PM, Peterson ED, Wang L, et al. Incidence of death and acute myocardial infarction associated with stopping clopidogrel after acute coronary syndrome. JAMA. 2008 Feb 6;299(5):532–539. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
