

The role of thyroid eye disease and other factors in the overcorrection of hypotropia following unilateral adjustable suture recession of the inferior rectus (an American Ophthalmological Society thesis)
- PMID: 22253487
- PMCID: PMC3259676
The role of thyroid eye disease and other factors in the overcorrection of hypotropia following unilateral adjustable suture recession of the inferior rectus (an American Ophthalmological Society thesis)
Abstract
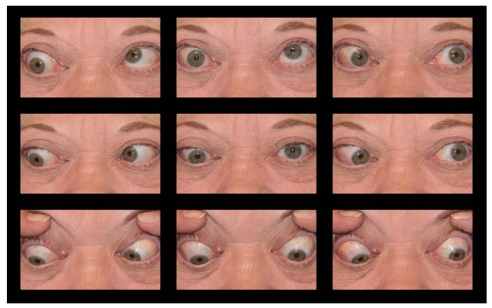
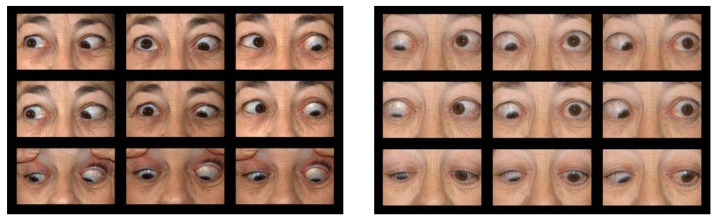
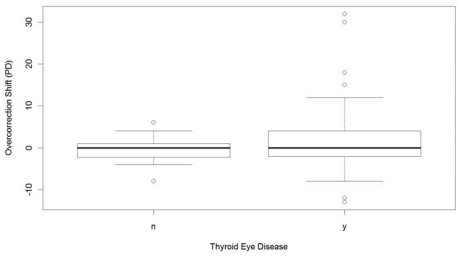
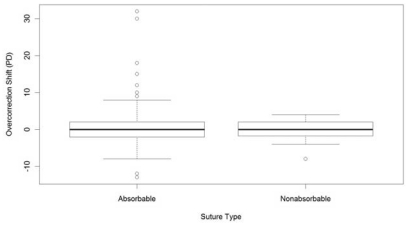
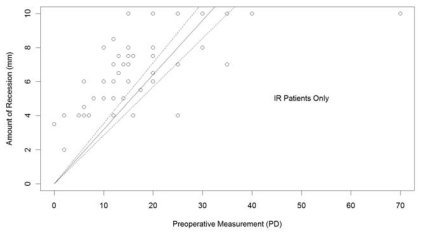
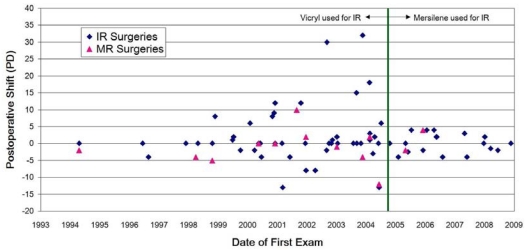
Purpose: Overcorrection of hypotropia subsequent to adjustable suture surgery following inferior rectus recession is undesirable, often resulting in persistent diplopia and reoperation. I hypothesized that overcorrection shift after suture adjustment may be unique to thyroid eye disease, and the use of a nonabsorbable suture may reduce the occurrence of overcorrection.
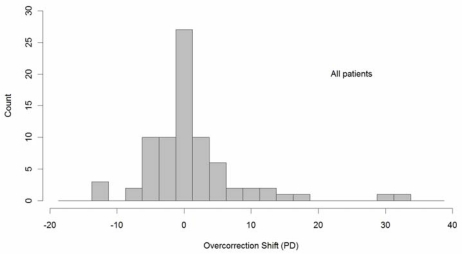
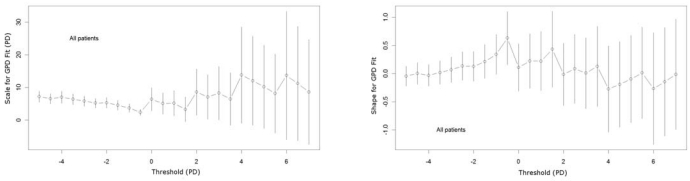
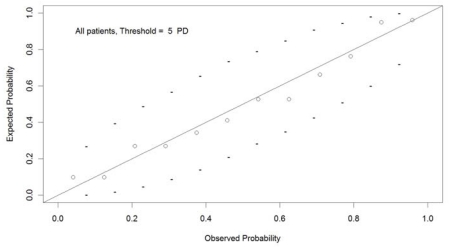
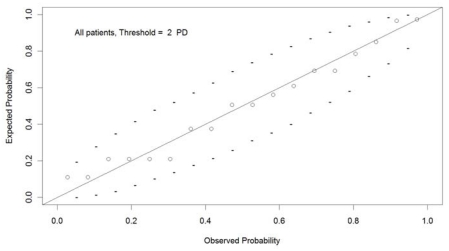
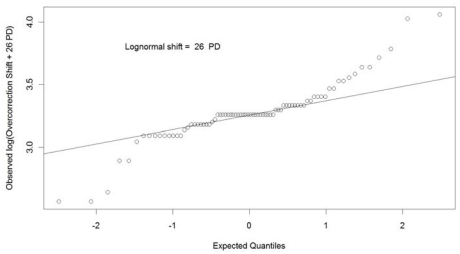
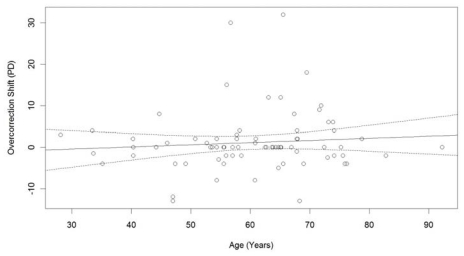
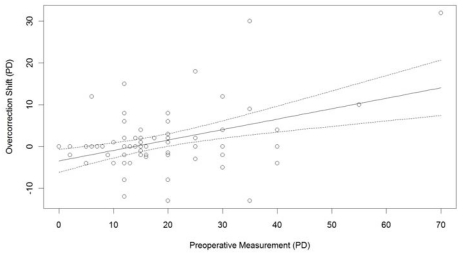
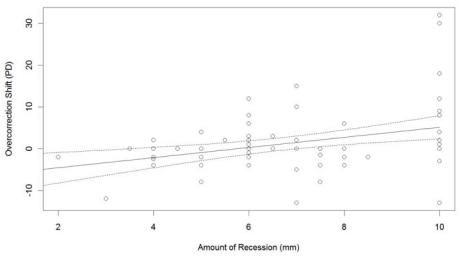
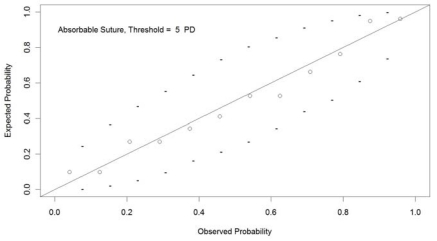
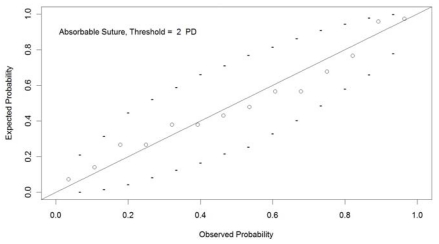
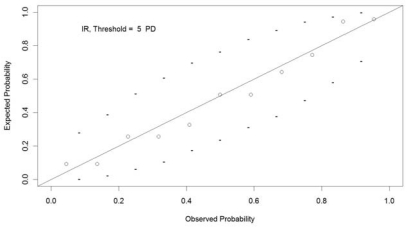
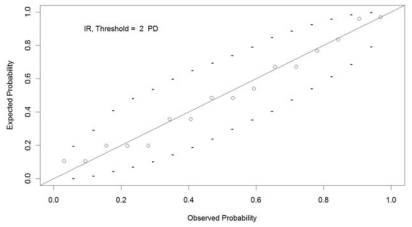
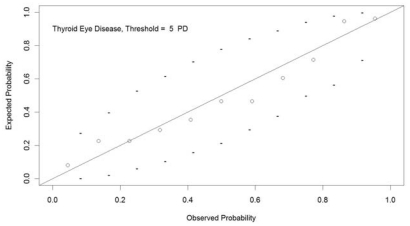
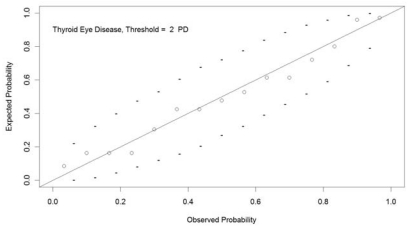
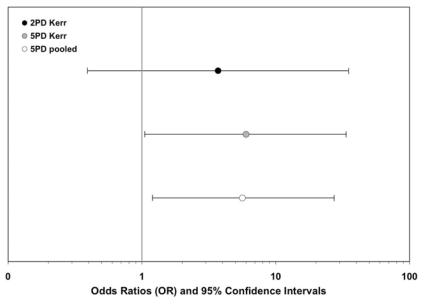
Methods: A retrospective chart review of adult patients who had undergone eye muscle surgery with an adjustable suture technique was performed. Overcorrection shifts that occurred between the time of suture adjustment and 2 months postoperatively were examined. Descriptive statistics, linear regression, Anderson-Darling tests, generalized Pareto distributions, odds ratios, and Fisher tests were performed for two overcorrection shift thresholds (>2 and >5 prism diopters [PD]).
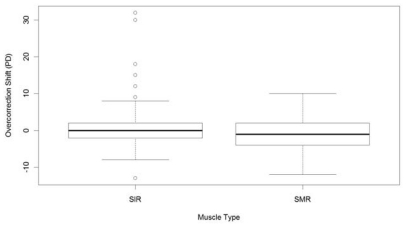
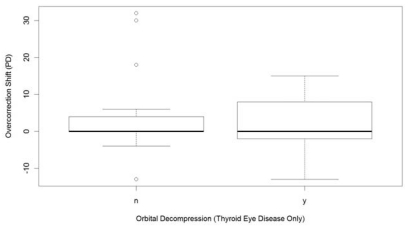
Results: Seventy-seven patients were found: 34 had thyroid eye disease and inferior rectus recession, 30 had no thyroid eye disease and inferior rectus recession, and 13 patients had thyroid eye disease and medial rectus recession. Eighteen cases exceeded the 2 PD threshold, and 12 exceeded the 5 PD threshold. Statistical analyses indicated that overcorrection was associated with thyroid eye disease (P=6.7E-06), inferior rectus surgery (P=6.7E-06), and absorbable sutures (>2 PD: OR=3.7, 95% CI=0.4-35.0, P=0.19; and >5 PD: OR=6.0, 95% CI=1.1-33.5, P=0.041).
Conclusions: After unilateral muscle recession for hypotropia, overcorrection shifts are associated with thyroid eye disease, surgery of the inferior rectus, and use of absorbable sutures. Surgeons performing unilateral inferior rectus recession on adjustable suture in the setting of thyroid eye disease should consider using a nonabsorbable suture to reduce the incidence of postoperative overcorrection.
Figures
Similar articles
-
Postoperative shift in ocular alignment following single vertical rectus recession on adjustable suture in adults without thyroid eye disease.J AAPOS. 2015 Jun;19(3):247-51. doi: 10.1016/j.jaapos.2015.03.015. J AAPOS. 2015. PMID: 26059671
-
Surgical management of vertical ocular misalignment in thyroid eye disease using an adjustable suture technique.J AAPOS. 2012 Dec;16(6):518-22. doi: 10.1016/j.jaapos.2012.08.010. J AAPOS. 2012. PMID: 23237747
-
Overcorrection after adjustable suture suspension- recession of the inferior rectus muscle in non-thyroid eye disease.Binocul Vis Strabismus Q. 1999;14(2):103-6. Binocul Vis Strabismus Q. 1999. PMID: 10506686
-
Bilateral inferior rectus muscle recession for correction of hypotropia in dysthyroid ophthalmopathy.J AAPOS. 1999 Jun;3(3):157-9. doi: 10.1016/s1091-8531(99)70061-3. J AAPOS. 1999. PMID: 10428589
-
Management of strabismus in thyroid eye disease.Eye (Lond). 2015 Feb;29(2):234-7. doi: 10.1038/eye.2014.282. Epub 2014 Dec 19. Eye (Lond). 2015. PMID: 25523204 Free PMC article. Review.
Cited by
-
Outcomes of the intraoperative relaxed muscle positioning technique in strabismus surgery for thyroid eye disease.Pediatr Investig. 2025 Feb 25;9(2):133-138. doi: 10.1002/ped4.12467. eCollection 2025 Jun. Pediatr Investig. 2025. PMID: 40539016 Free PMC article. Review.
-
Surgical Responses of Medial Rectus Muscle Recession in Thyroid Eye Disease-Related Esotropia.PLoS One. 2016 Jan 21;11(1):e0146779. doi: 10.1371/journal.pone.0146779. eCollection 2016. PLoS One. 2016. PMID: 26796354 Free PMC article.
-
Clinical Pearls and Management Recommendations for Strabismus due to Thyroid Orbitopathy.Middle East Afr J Ophthalmol. 2015 Jul-Sep;22(3):307-11. doi: 10.4103/0974-9233.159731. Middle East Afr J Ophthalmol. 2015. PMID: 26180468 Free PMC article. Review.
-
Management of Thyroid Eye Disease-Related Strabismus.J Curr Ophthalmol. 2020 Mar 23;32(1):1-13. doi: 10.1016/j.joco.2019.10.002. eCollection 2020 Jan-Mar. J Curr Ophthalmol. 2020. PMID: 32510007 Free PMC article. Review.
-
Adjustable Versus Nonadjustable Sutures in Strabismus Surgery-Who Benefits the Most?J Clin Med. 2020 Jan 21;9(2):292. doi: 10.3390/jcm9020292. J Clin Med. 2020. PMID: 31973012 Free PMC article. Review.
References
-
- Metz HS. Strabismus related to Graves ophthalmopathy. In: Rosenbaum AL, Santiago AP, editors. Clinical Strabismus Management: Principles and Surgical Techniques. Philadelphia: WB Saunders; 1999. pp. 285–295.
-
- Parry CH. Collections From Unpublished Medical Writings of the Late Caleb Hiller Parry MD FRS. Vol. 2. London: Underwoods; 1825.
-
- Von Basedow CA. Exophthalmos durch Hypertrophie des Zellgewebes in der Augenhohle. Wochenschr Ges Heilkd. 1840;6:197.
-
- Von Graefe A. Bemerkiengen uber Exophthalmos mit Struma und Herzleiten. Von Graefes Arch Ophthalmol. 1857;3:278.
-
- Loeb L, Friedman H. Exophthalmos produced by injection of acid extract of anterior pituitary gland of cattle. Proc Soc Exp Biol. 1932;29:648.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
