

Genome-wide high-resolution aCGH analysis of gestational choriocarcinomas
- PMID: 22253721
- PMCID: PMC3253784
- DOI: 10.1371/journal.pone.0029426
Genome-wide high-resolution aCGH analysis of gestational choriocarcinomas
Abstract
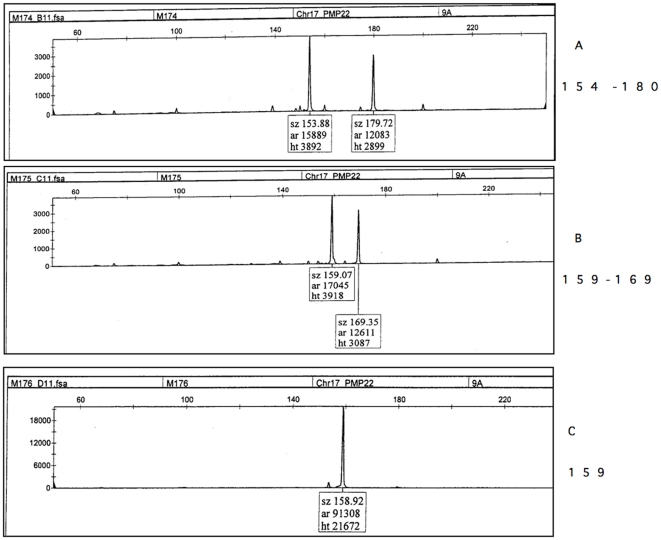
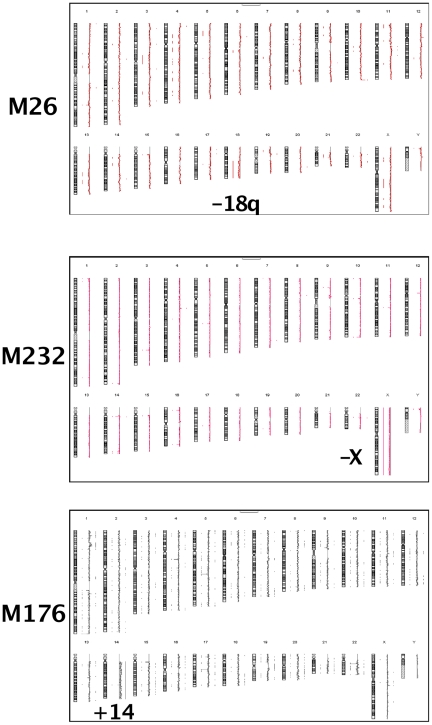
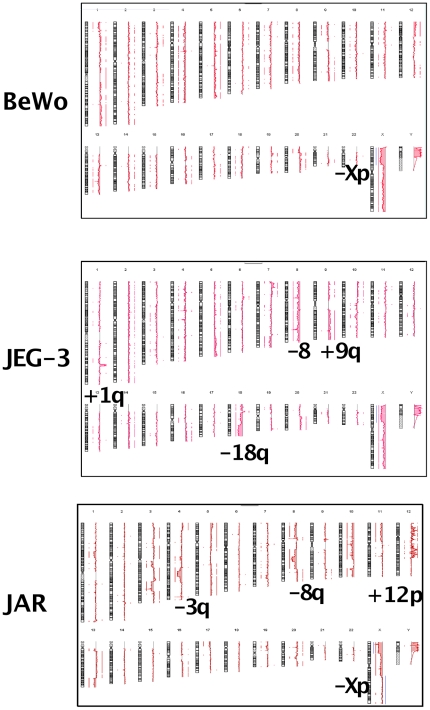
Eleven samples of DNA from choriocarcinomas were studied by high resolution CGH-array 244 K. They were studied after histopathological confirmation of the diagnosis, of the androgenic etiology and after a microsatellite marker analysis confirming the absence of contamination of tumor DNA from maternal DNA. Three cell lines, BeWo, JAR, JEG were also studied by this high resolution pangenomic technique. According to aCGH analysis, the de novo choriocarcinomas exhibited simple chromosomal rearrangements or normal profiles. The cell lines showed various and complex chromosomal aberrations. 23 Minimal Critical Regions were defined that allowed us to list the genes that were potentially implicated. Among them, unusually high numbers of microRNA clusters and imprinted genes were observed.
Conflict of interest statement
Figures
Similar articles
-
[Cytogenomic studies of hydatiform moles and gestational choriocarcinoma].Bull Cancer. 2012 Sep;99(9):827-43. doi: 10.1684/bdc.2012.1621. Bull Cancer. 2012. PMID: 22877883 French.
-
Detection of non-maternal components of gestational choriocarcinoma by PCR-based microsatellite DNA assay.Gynecol Oncol. 2006 Nov;103(2):614-7. doi: 10.1016/j.ygyno.2006.04.008. Epub 2006 Jun 5. Gynecol Oncol. 2006. PMID: 16740299
-
Genomic profile in gestational and non-gestational choriocarcinomas.Placenta. 2017 Feb;50:8-15. doi: 10.1016/j.placenta.2016.12.009. Epub 2016 Dec 7. Placenta. 2017. PMID: 28161066
-
Zoom-in array comparative genomic hybridization (aCGH) to detect germline rearrangements in cancer susceptibility genes.Methods Mol Biol. 2010;653:221-35. doi: 10.1007/978-1-60761-759-4_13. Methods Mol Biol. 2010. PMID: 20721746 Review.
-
[CGH (comparative genomic hybridization)].Nihon Rinsho. 1996 Apr;54(4):933-43. Nihon Rinsho. 1996. PMID: 8920653 Review. Japanese.
Cited by
-
Differential expression of E-cadherin, β-catenin, and Lewis x between invasive hydatidiform moles and post-molar choriocarcinomas.Virchows Arch. 2013 Jun;462(6):653-63. doi: 10.1007/s00428-013-1427-z. Epub 2013 May 17. Virchows Arch. 2013. PMID: 23681114
-
Sensitive screening of single nucleotide polymorphisms in cell free DNA for diagnosis of gestational tumours.NPJ Genom Med. 2022 Apr 8;7(1):26. doi: 10.1038/s41525-022-00297-x. NPJ Genom Med. 2022. PMID: 35396509 Free PMC article.
-
Inherent mosaicism and extensive mutation of human placentas.Nature. 2021 Apr;592(7852):80-85. doi: 10.1038/s41586-021-03345-1. Epub 2021 Mar 10. Nature. 2021. PMID: 33692543 Free PMC article.
-
Embryonal Fyn-associated substrate (EFS) and CASS4: The lesser-known CAS protein family members.Gene. 2015 Oct 1;570(1):25-35. doi: 10.1016/j.gene.2015.06.062. Epub 2015 Jun 26. Gene. 2015. PMID: 26119091 Free PMC article. Review.
-
Altered p16 and Bcl-2 expression reflects pathologic development in hydatidiform moles and choriocarcinoma.Pathol Oncol Res. 2013 Apr;19(2):217-27. doi: 10.1007/s12253-012-9572-2. Epub 2012 Oct 13. Pathol Oncol Res. 2013. PMID: 23065465
References
-
- Philippe E, Boue J, Boue A. [Trophoblastic gestational diseases. Triploid syndrome, perivillous trophoblastic hyperplasia, trophoblastic pseudotumor, trophoblastic microcarcinoma and carcinoma]. Ann Anat Pathol (Paris) 1980;25:13–38. - PubMed
-
- Kajii T, Ohama K. Sporadic triploid and hexaploid cells in embryonic tissue. Negative relationship to maternal intake of oral contraceptives. Ann Genet. 1972;15:11–18. - PubMed
-
- Jacobs PA, Szulman AE, Funkhouser J, Matsuura JS, Wilson CC. Human triploidy: relationship between parental origin of the additional haploid complement and development of partial hydatidiform mole. Ann Hum Genet. 1982;46:223–231. - PubMed
-
- Deveault C, Qian JH, Chebaro W, Ao A, Gilbert L, et al. NLRP7 mutations in women with diploid androgenetic and triploid moles: a proposed mechanism for mole formation. Hum Mol Genet. 2009;18:888–897. - PubMed
-
- Wang CM, Dixon PH, Decordova S, Hodges MD, Sebire NJ, et al. Identification of 13 novel NLRP7 mutations in 20 families with recurrent hydatidiform mole; missense mutations cluster in the leucine-rich region. J Med Genet. 2009;46:569–575. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
