

Orientia tsutsugamushi in human scrub typhus eschars shows tropism for dendritic cells and monocytes rather than endothelium
- PMID: 22253938
- PMCID: PMC3254662
- DOI: 10.1371/journal.pntd.0001466
Orientia tsutsugamushi in human scrub typhus eschars shows tropism for dendritic cells and monocytes rather than endothelium
Abstract
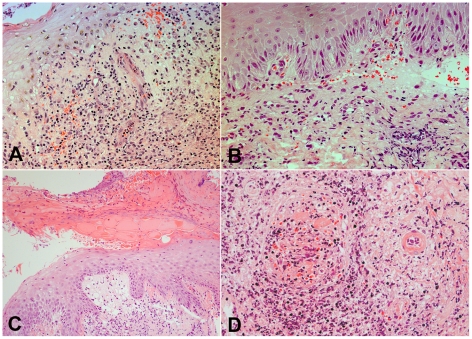
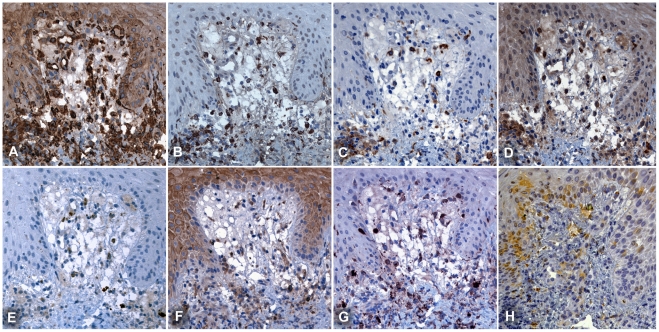
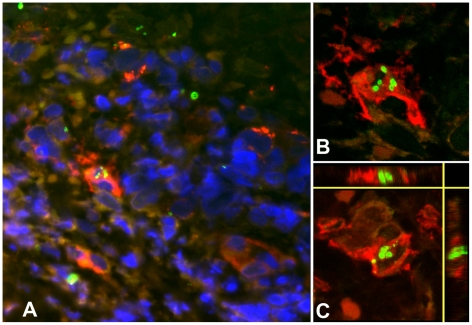
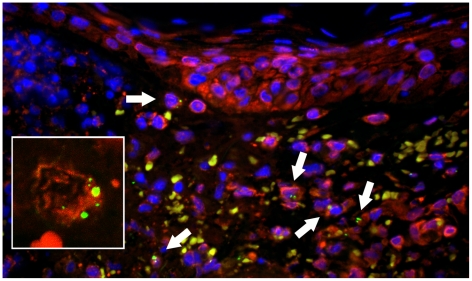
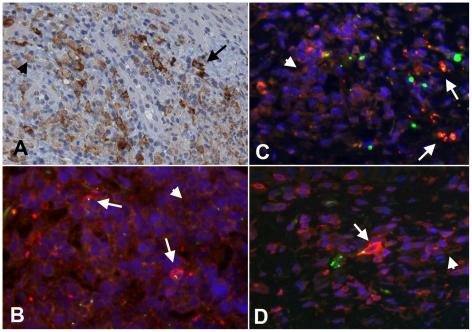
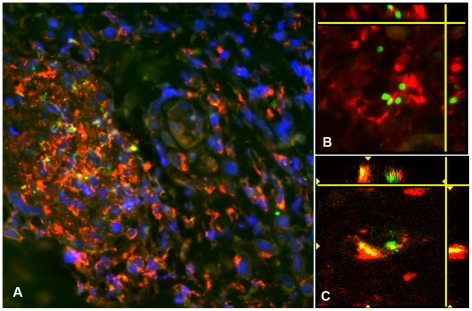
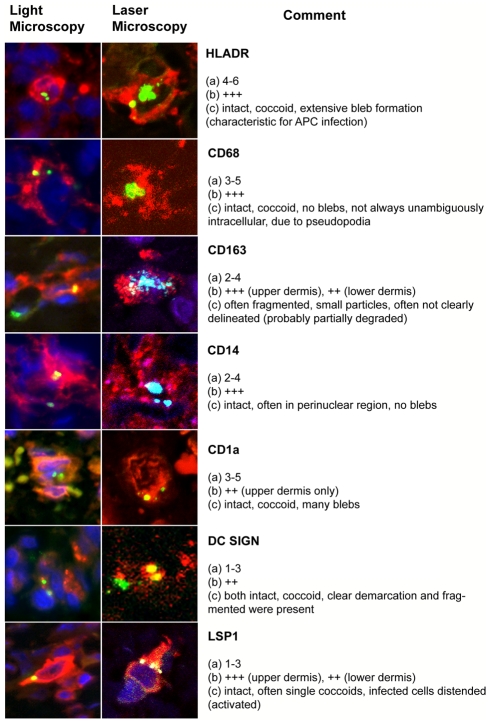
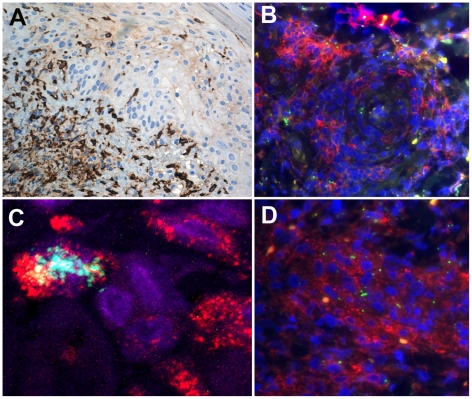
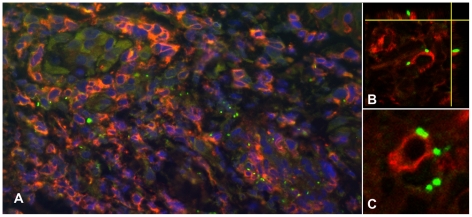
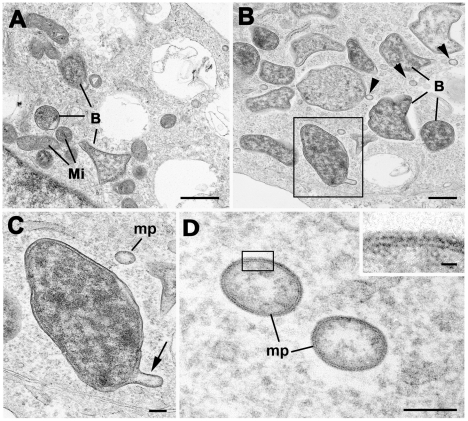
Scrub typhus is a common and underdiagnosed cause of febrile illness in Southeast Asia, caused by infection with Orientia tsutsugamushi. Inoculation of the organism at a cutaneous mite bite site commonly results in formation of a localized pathological skin reaction termed an eschar. The site of development of the obligate intracellular bacteria within the eschar and the mechanisms of dissemination to cause systemic infection are unclear. Previous postmortem and in vitro reports demonstrated infection of endothelial cells, but recent pathophysiological investigations of typhus patients using surrogate markers of endothelial cell and leucocyte activation indicated a more prevalent host leucocyte than endothelial cell response in vivo. We therefore examined eschar skin biopsies from patients with scrub typhus to determine and characterize the phenotypes of host cells in vivo with intracellular infection by O. tsutsugamushi, using histology, immunohistochemistry, double immunofluorescence confocal laser scanning microscopy and electron microscopy. Immunophenotyping of host leucocytes infected with O. tsutsugamushi showed a tropism for host monocytes and dendritic cells, which were spatially related to different histological zones of the eschar. Infected leucocyte subsets were characterized by expression of HLADR+, with an "inflammatory" monocyte phenotype of CD14/LSP-1/CD68 positive or dendritic cell phenotype of CD1a/DCSIGN/S100/FXIIIa and CD163 positive staining, or occasional CD3 positive T-cells. Endothelial cell infection was rare, and histology did not indicate a widespread inflammatory vasculitis as the cause of the eschar. Infection of dendritic cells and activated inflammatory monocytes offers a potential route for dissemination of O. tsutsugamushi from the initial eschar site. This newly described cellular tropism for O. tsutsugamushi may influence its interaction with local host immune responses.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Rosenberg R. Drug-resistant scrub typhus: Paradigm and paradox. Parasitol Today. 1997;13:131–132. - PubMed
-
- Blacksell SD, Bryant NJ, Paris DH, Doust JA, Sakoda Y, et al. Scrub typhus serologic testing with the indirect immunofluorescence method as a diagnostic gold standard: a lack of consensus leads to a lot of confusion. Clin Infect Dis. 2007;44:391–401. - PubMed
-
- Lee YS, Wang PH, Tseng SJ, Ko CF, Teng HJ. Epidemiology of scrub typhus in eastern Taiwan, 2000–2004. Jpn J Infect Dis. 2006;59:235–238. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
