

Targeting cardiac fibrosis: a new frontier in antiarrhythmic therapy?
- PMID: 22254191
- PMCID: PMC3253497
Targeting cardiac fibrosis: a new frontier in antiarrhythmic therapy?
Abstract
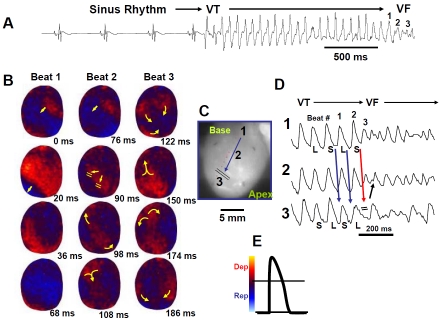
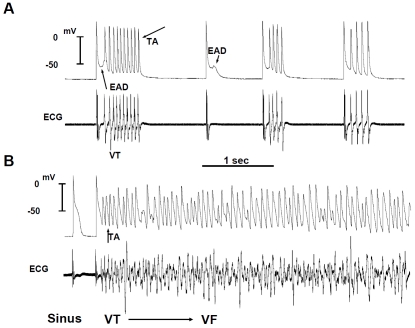
Cardiac fibrosis is known to alter cardiac conduction and promote reentry. Recent evidence indicates that fibrosis characterized by increased interstitial collagen accumulation and increased myofibroblast proliferation also promotes enhanced automaticity and early afterdepolarizations (EADs) causing triggered activity. Fibrosis then becomes an effective therapeutic target for the management of lethal cardiac arrhythmias. While oxidative stress with hydrogen peroxide (H(2)O(2)) is shown to readily promote EADs and triggered activity in isolated rat and rabbit ventricular myocytes however, this same stress fails to cause EADs in well-coupled, non-fibrotic hearts due to source-to-sink mismatches arising from cell-to-cell coupling. The triggered activity in the aged fibrotic hearts causes focal ventricular tachycardia (VT) that degenerates within seconds to ventricular fibrillation (VF) after the emergence of spatially discordant action potential duration alternans leading to wavebreak, reentry and VF. Computer simulations in 2D tissue incorporating variable degrees of fibrosis showed that intermediate (but not mild or very severe) fibrosis promoted EADs and TA. Human studies have shown that myocardial fibrosis was an independent predictor for arrhythmias including sustained VT and VF. A variety of drug classes including, torsemide, a loop diuretic, that inhibits the enzyme involved in the myocardial extracellular generation of collagen type I molecules and the inhibitors of the renin-angiotensin-aldosterone system (RAAS), the mineralocorticoid receptors and endothelin receptors reduce cardiac fibrosis with reduction of myocardial stiffness and improved ventricular function. It is hoped that in the near future effective antifibrotic drug regimen would be developed to reduce the risk of fibrosis related VT and VF.
Keywords: Early afterdepolarization; discordant alternans; fibrosis; myofibroblast; optical mapping; oxidative stress; triggered activity; ventricular fibrillation; ventricular tachycardia.
Figures
References
-
- Spach MS, Boineau JP. Microfibrosis produces electrical load variations due to loss of side-to-side cell connections: a major mechanism of structural heart disease arrhythmias. Pacing Clin Electrophysiol. 1997;20:397–413. - PubMed
-
- Spach MS, Dolber PC. Relating extracellular potentials and their derivatives to anisotropic propagation at a microscopic level in human cardiac muscle. Evidence for electrical uncoupling of side-to-side fiber connections with increasing age. Circ Res. 1986;58:356–371. - PubMed
-
- de Bakker JM, van Capelle FJ, Janse MJ, Tasseron S, Vermeulen JT, de Jonge N, Lahpor JR. Slow conduction in the infarcted human heart. ‘Zigzag’ course of activation. Circulation. 1993;88:915–926. - PubMed
-
- Wu TJ, Ong JJ, Hwang C, Lee JJ, Fishbein MC, Czer L, Trento A, Blanche C, Kass RM, Mandel WJ, Karagueuzian HS, Chen PS. Characteristics of wave fronts during ventricular fibrillation in human hearts with dilated cardiomyopathy: role of increased fibrosis in the generation of reentry. J Am Coll Cardiol. 1998;32:187–196. - PubMed
-
- de Bakker JMT, Coronel R, Tasseron S, Wilde AAM, Opthof T, Janse MJ, van Capelle FJL, Becker AE, Jambroes G. Ventricular tachycardia in the infarcted, Langendorff-perfused human heart: Role of the arrangement of surviving cardiac fibers. J Am Coll Cardiol. 1990;15:1594–1607. - PubMed
LinkOut - more resources
Full Text Sources