

Abnormal baroreflex function is dissociated from central angiotensin II receptor expression in chronic heart failure
- PMID: 22258229
- PMCID: PMC3281308
- DOI: 10.1097/SHK.0b013e31824581e8
Abnormal baroreflex function is dissociated from central angiotensin II receptor expression in chronic heart failure
Abstract
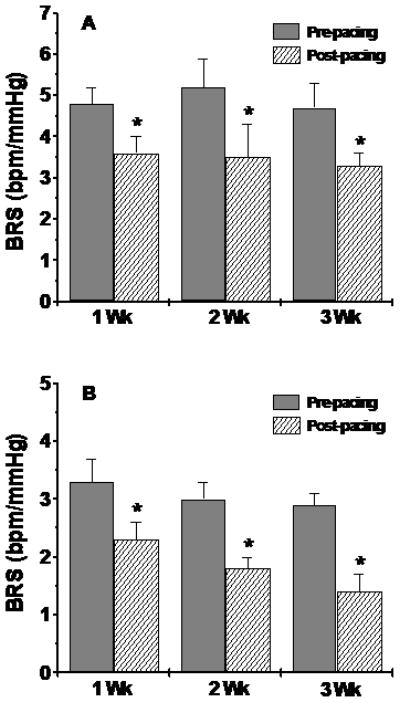
Neurohumoral disturbances characterize chronic heart failure (CHF) and are reflected, in part, as impairment of baroreflex sensitivity (BRS) and sympathetic function. However, the mechanisms that trigger these neurohumoral abnormalities in CHF are not clear. We hypothesized that the BRS is blunted early in CHF and that the humoral effects occur later and contribute to progressive loss of cardiovascular control in CHF. We assessed the BRS (beats/min per mmHg) and recorded renal sympathetic nerve activity (RSNA) in four groups of conscious rabbits at varying time intervals: control, 1-week CHF, 2-week CHF, and 3-week CHF. Chronic heart failure was induced by ventricular pacing at 360 beats/min and was assessed by echocardiography. Arterial blood pressure and heart rate were recorded by an implanted telemetric device and RSNA through an implanted electrode. A significant fall in the ejection fraction, fractional shortening, and an increase in left ventricular end-systolic diameter and left ventricular end-diastolic diameter were observed in all CHF groups. The BRS was significantly reduced in all the CHF groups with no significant change in the basal RSNA (% of maximum) after 1 week of pacing; a small but insignificant rise in RSNA was seen at 2 weeks, and a significant rise in RSNA was observed at 3 weeks. Angiotensin II type 1 (AT-1) receptor protein (Western Blot) and mRNA (reverse transcriptase-polymerase chain reaction) expression in the rostral ventrolateral medulla exhibited a progressive increase with the duration of CHF, reaching significance after 3 weeks, the same time point in which RSNA was significantly elevated. These data are the first to examine early changes in central AT-1 receptors in CHF and suggest that the fall in BRS and hemodynamic changes occur early in the development of CHF followed by sympathoexcitation and overexpression of AT-1 receptors with the progression of CHF, causing further impairment of cardiovascular control.
Figures



References
-
- DiBona GF, Jones SY, Brooks VL. ANG II receptor blockade and arterial baroreflex regulation of renal nerve activity in cardiac failure. Am J Physiol. 1995;69:R1189–R1196. - PubMed
-
- Gao L, Wang W, Li YL, Schultz HD, Liu D, Cornish KG, Zucker IH. Sympatho-excitation by central Ang II: The roles for AT1 receptor upregulation and NAD(P)H oxidase in the RVLM. Am J Physiol Heart Circ Physiol. 2005;288:H2271–H2279. - PubMed
-
- Kaye DM, Lefkovits J, Cox H, Lambert G, Jennings G, Turner A, Esler MD. Regional epinephrine kinetics in human heart failure: evidence for extra-adrenal, nonneural release. Am J Physiol. 1995;269:H182–H188. - PubMed
-
- Svanegaard J, Johansen JB, Thayssen P, et al. Neurohormonal systems during progression of heart failure: A review. Cardiology. 1993;83:21–29. - PubMed
-
- Wollert KC, Drexler H. The renin-angiotensin system and experimental heart failure. Cardiov Res. 1999;43:838–849. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
