

Treatment patterns and health care resource utilization in a 1-year observational cohort study of outpatients with schizophrenia at risk of nonadherence treated with long-acting injectable antipsychotics
- PMID: 22259237
- PMCID: PMC3259075
- DOI: 10.2147/PPA.S26253
Treatment patterns and health care resource utilization in a 1-year observational cohort study of outpatients with schizophrenia at risk of nonadherence treated with long-acting injectable antipsychotics
Abstract
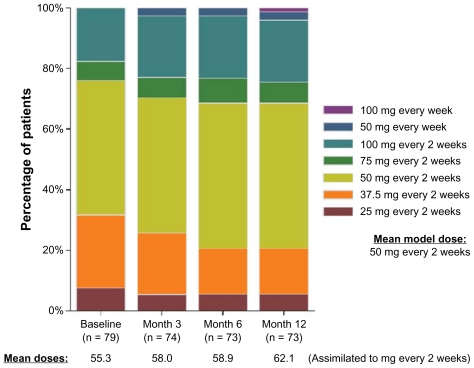
Purpose: To describe (1) the clinical profiles and the patterns of use of long-acting injectable (LAI) antipsychotics in patients with schizophrenia at risk of nonadherence with oral antipsychotics, and in those who started treatment with LAI antipsychotics, (2) health care resource utilization and associated costs.
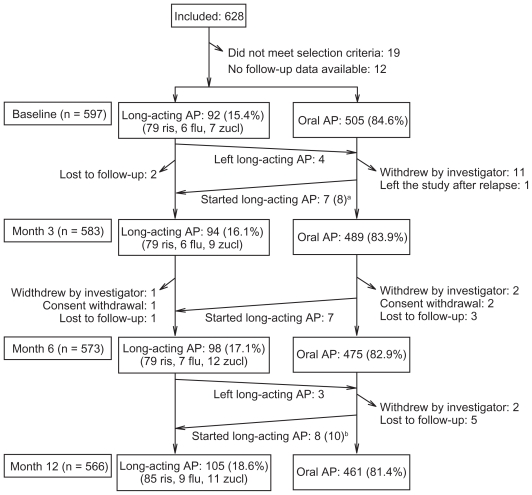
Patients and methods: A total of 597 outpatients with schizophrenia at risk of nonadherence, according to the psychiatrist's clinical judgment, were recruited at 59 centers in a noninterventional prospective observational study of 1-year follow-up when their treatment was modified. In a post hoc analysis, the profiles of patients starting LAI or continuing with oral antipsychotics were described, and descriptive analyses of treatments, health resource utilization, and direct costs were performed in those who started an LAI antipsychotic.
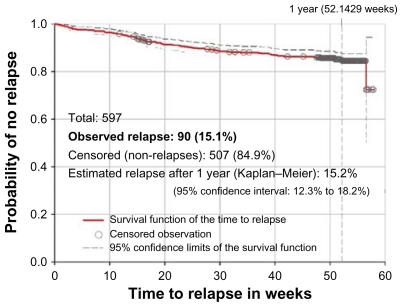
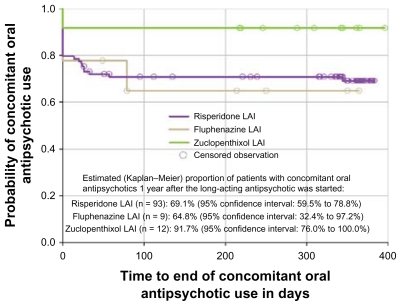
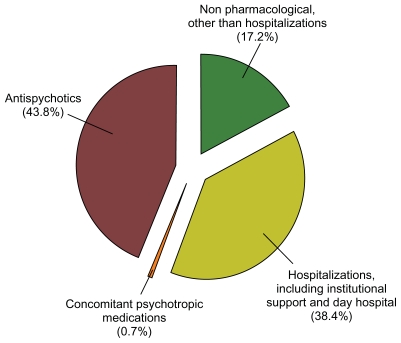
Results: Therapy modifications involved the antipsychotic medications in 84.8% of patients, mostly because of insufficient efficacy of prior regimen. Ninety-two (15.4%) patients started an LAI antipsychotic at recruitment. Of these, only 13 (14.1%) were prescribed with first-generation antipsychotics. During 1 year, 16.3% of patients who started and 14.9% of patients who did not start an LAI antipsychotic at recruitment relapsed, contrasting with the 20.9% who had been hospitalized only within the prior 6 months. After 1 year, 74.3% of patients who started an LAI antipsychotic continued concomitant treatment with oral antipsychotics. The mean (median) total direct health care cost per patient per month during the study year among the patients starting any LAI antipsychotic at baseline was €1,407 (€897.7). Medication costs (including oral and LAI antipsychotics and concomitant medication) represented almost 44%, whereas nonmedication costs accounted for more than 55% of the mean total direct health care costs.
Conclusion: LAI antipsychotics were infrequently prescribed in spite of a psychiatrist-perceived risk of nonadherence to oral antipsychotics. Mean medication costs were lower than nonmedication costs.
Keywords: depot preparations; health care costs; medication adherence.
Figures
Similar articles
-
Treatment Patterns, Healthcare Resource Utilization and Costs Among Schizophrenia Patients Treated with Long-Acting Injectable Versus Oral Antipsychotics.Adv Ther. 2018 Nov;35(11):1994-2014. doi: 10.1007/s12325-018-0786-x. Epub 2018 Sep 29. Adv Ther. 2018. PMID: 30269292
-
Treatment Patterns, Health Care Resource Utilization, and Spending in Medicaid Beneficiaries Initiating Second-generation Long-acting Injectable Agents Versus Oral Atypical Antipsychotics.Clin Ther. 2017 Oct;39(10):1972-1985.e2. doi: 10.1016/j.clinthera.2017.08.008. Epub 2017 Sep 15. Clin Ther. 2017. PMID: 28919292
-
[Cost-effectiveness analysis of schizophrenic patient care settings: impact of an atypical antipsychotic under long-acting injection formulation].Encephale. 2005 Mar-Apr;31(2):235-46. doi: 10.1016/s0013-7006(05)82390-5. Encephale. 2005. PMID: 15959450 Review. French.
-
Clinical and economic impact of long-acting injectable antipsychotics in patients previously treated with short-acting oral antipsychotics.J Manag Care Spec Pharm. 2022 Oct;28(10):1130-1137. doi: 10.18553/jmcp.2022.28.10.1130. J Manag Care Spec Pharm. 2022. PMID: 36125056 Free PMC article.
-
Converting oral to long-acting injectable antipsychotics: a guide for the perplexed.CNS Spectr. 2017 Dec;22(S1):14-28. doi: 10.1017/S1092852917000840. CNS Spectr. 2017. PMID: 29350127 Review.
Cited by
-
Impact of schizophrenia relapse definition on the comparative effectiveness of oral versus injectable antipsychotics: A systematic review and meta-analysis of observational studies.Pharmacol Res Perspect. 2022 Feb;10(1):e00915. doi: 10.1002/prp2.915. Pharmacol Res Perspect. 2022. PMID: 35089656 Free PMC article.
-
Multi-level barriers and facilitators to implementing evidence-based antipsychotics in the treatment of early-phase schizophrenia.Front Health Serv. 2024 Oct 14;4:1385398. doi: 10.3389/frhs.2024.1385398. eCollection 2024. Front Health Serv. 2024. PMID: 39469435 Free PMC article.
-
Healthcare cost reductions associated with the use of LAI formulations of antipsychotic medications versus oral among patients with schizophrenia.J Behav Health Serv Res. 2013 Jul;40(3):355-66. doi: 10.1007/s11414-013-9329-z. J Behav Health Serv Res. 2013. PMID: 23579871
References
-
- Lacro JP, Dunn LB, Dolder CR, Leckband SG, Jeste DV. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892–909. - PubMed
-
- Ascher-Svanum H, Faries DE, Zhu B, Ernst FR, Swartz MS, Swanson JW. Medication adherence and long-term functional outcomes in the treatment of schizophrenia in usual care. J Clin Psychiatry. 2006;67(3):453–460. - PubMed
-
- Law MR, Soumerai SB, Ross-Degnan D, Adams AS. A longitudinal study of medication nonadherence and hospitalization risk in schizophrenia. J Clin Psychiatry. 2008;69(1):47–53. - PubMed
-
- Lieberman JA, Stroup TS, McEvoy JP, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia [published correction appears in N Engl J Med. 2010;363(11):1092–1093] N Engl J Med. 2005;353(12):1209–1223. - PubMed
-
- Mueser KT, McGurk SR. Schizophrenia. Lancet. 2004;363(9426):2063–2072. - PubMed
