Right ventricular compression observed in echocardiography from pectus excavatum deformity
- PMID: 22259662
- PMCID: PMC3259543
- DOI: 10.4250/jcu.2011.19.4.192
Right ventricular compression observed in echocardiography from pectus excavatum deformity
Abstract
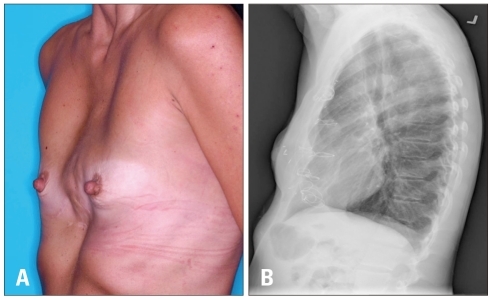
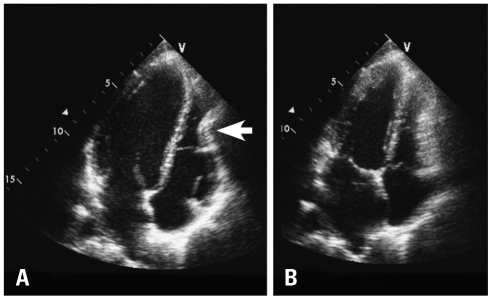
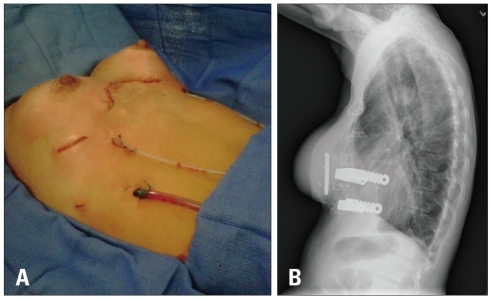
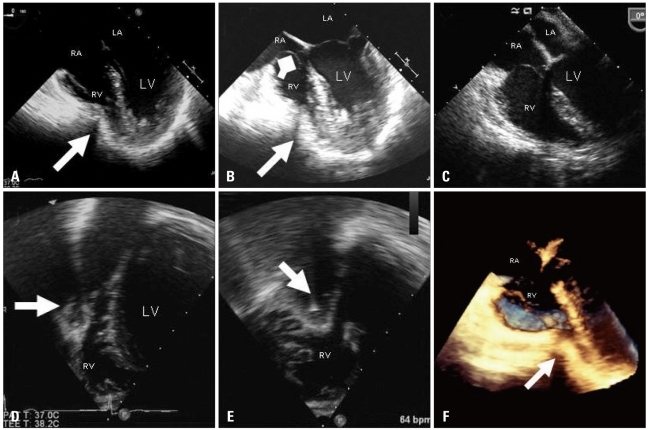
Pectus excavatum exists as varying anatomic deformities and compression of the right heart by the chest wall can lead to patient symptoms including dyspnea and chest pain with exertion. Echocardiography can be difficult but is critical to the evaluation and diagnosis of this patient population. Modifying standard views such as biplane transthoracic and 3-D transesophageal views may be necessary in some patients due to limitations from the abnormal anatomy of the deformed anterior chest wall. Apical four-chamber views when seen clearly can usually visualize any extrinsic compression to the right ventricle of the heart.
Keywords: Chest pain; Chest wall deformity; Echocardiography right heart; Pectus excavatum; Right ventricular compression.
Figures

References
-
- Heinle J, Sabiston DC., Jr . Congenital deformities of the chest wall. In: Sabiston DC Jr, Lyerly HK, editors. Textbook of surgery: the biological basis of modern surgical practice. 15th ed. Philadelphia: WB Saunders Co; 1997. pp. 1888–1896.
-
- Fokin AA, Steuerwald NM, Ahrens WA, Allen KE. Anatomical, histologic, and genetic characteristics of congenital chest wall deformities. Semin Thorac Cardiovasc Surg. 2009;21:44–57. - PubMed
-
- Jaroszewski D, Notrica D, McMahon L, Steidley DE, Deschamps C. Current management of pectus excavatum: a review and update of therapy and treatment recommendations. J Am Board Fam Med. 2010;23:230–239. - PubMed
-
- Jaroszewski DE, Fonkalsrud EW. Repair of pectus chest deformities in 320 adult patients: 21 year experience. Ann Thorac Surg. 2007;84:429–433. - PubMed
-
- Jaroszewski D, Steidley E, Galindo A, Arabia F. Treating heart failure and dyspnea in a 78-year-old man with surgical correction of pectus excavatum. Ann Thorac Surg. 2009;88:1008–1010. - PubMed
Publication types
LinkOut - more resources
Full Text Sources