

Continence rate and oncological feasibility after total transurethral resection of the prostate as an alternative therapy for the treatment of prostate cancer: a pilot study
- PMID: 22259737
- PMCID: PMC3256308
- DOI: 10.5213/inj.2011.15.4.222
Continence rate and oncological feasibility after total transurethral resection of the prostate as an alternative therapy for the treatment of prostate cancer: a pilot study
Abstract
Purpose: The value of total transurethral resection of prostate cancer (TURPC) as an alternative therapy was first recognized by Hans J. Reuter. Thus, we conducted the study of prospectively collected data to verify total TURPC as an alternative therapy forlocalized prostate cancer.
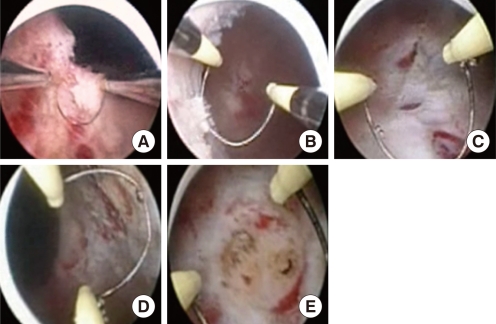
Methods: From January 2008 to July 2011, 14 patients with a mean age of 76.1 years (range, 66 to 89 years) with clinically localized prostate cancer were treated by prostatic resection by the corresponding author with curative intention.
Results: The mean duration of TURPC was 51.7 minutes (range, 30 to 120 minutes) and the mean amount of prostatic tissue resected was 21.2 g (range, 5 to 66 g). An intra- and/or postoperative blood transfusion was necessary in 2 cases. Hyponatremia was found in 7 patients. Six months after TURPC, 3 cases of grade 1 and 1 case of grade 2 incontinence were observed. Three patients in the high-risk group did not achieve a prostate specific antigen (PSA) nadir of ≤0.2 ng/mL. PSA recurrence occurred in one case in our series. Newly developed lymph node or distant metastases were not observed during the follow-up period.
Conclusions: According to our results, transurethral resection for prostate cancer can be performed with reasonable oncological results. The PSA nadir levels, and rates of biochemical failure and postoperative complications, including incontinence, were comparable with the published results for other procedures. TURPC is also inexpensive and non-invasive, and requires short hospitalization and a short surgical time without vesicourethral anastomosis.
Keywords: Prostate-specific antigen; Prostatic neoplasms; Transurethral resection of prostate; Urinary incontinence.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Aus G. Current status of HIFU and cryotherapy in prostate cancer--a review. Eur Urol. 2006;50:927–934. - PubMed
-
- Vallancien G, Prapotnich D, Cathelineau X, Baumert H, Rozet F. Transrectal focused ultrasound combined with transurethral resection of the prostate for the treatment of localized prostate cancer: feasibility study. J Urol. 2004;171(6 Pt 1):2265–2267. - PubMed
-
- Poissonnier L, Chapelon JY, Rouvière O, Curiel L, Bouvier R, Martin X, et al. Control of prostate cancer by transrectal HIFU in 227 patients. Eur Urol. 2007;51:381–387. - PubMed
-
- Blana A, Rogenhofer S, Ganzer R, Lunz JC, Schostak M, Wieland WF, et al. Eight years' experience with high-intensity focused ultrasonography for treatment of localized prostate cancer. Urology. 2008;72:1329–1333. - PubMed
-
- Babaian RJ, Donnelly B, Bahn D, Baust JG, Dineen M, Ellis D, et al. Best practice statement on cryosurgery for the treatment of localized prostate cancer. J Urol. 2008;180:1993–2004. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
