

Secondary cutaneous Epstein-Barr virus-associated diffuse large B-cell lymphoma in a patient with angioimmunoblastic T-cell lymphoma: a case report and review of literature
- PMID: 22260632
- PMCID: PMC3285033
- DOI: 10.1186/1746-1596-7-7
Secondary cutaneous Epstein-Barr virus-associated diffuse large B-cell lymphoma in a patient with angioimmunoblastic T-cell lymphoma: a case report and review of literature
Abstract
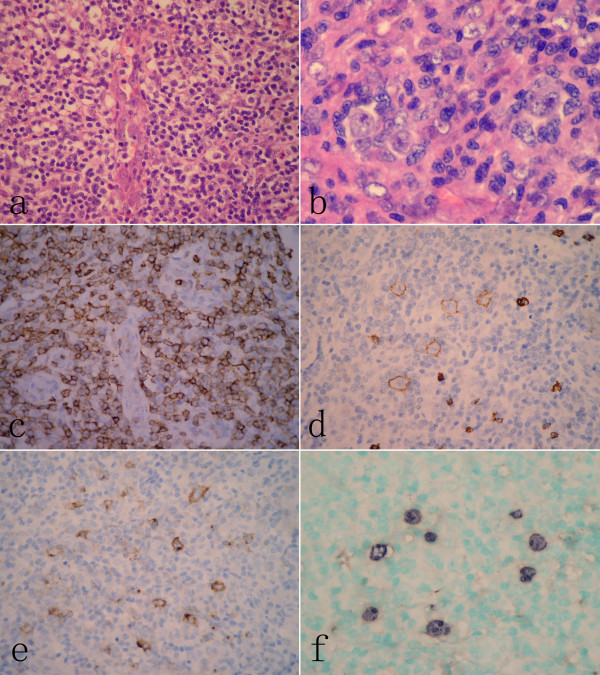
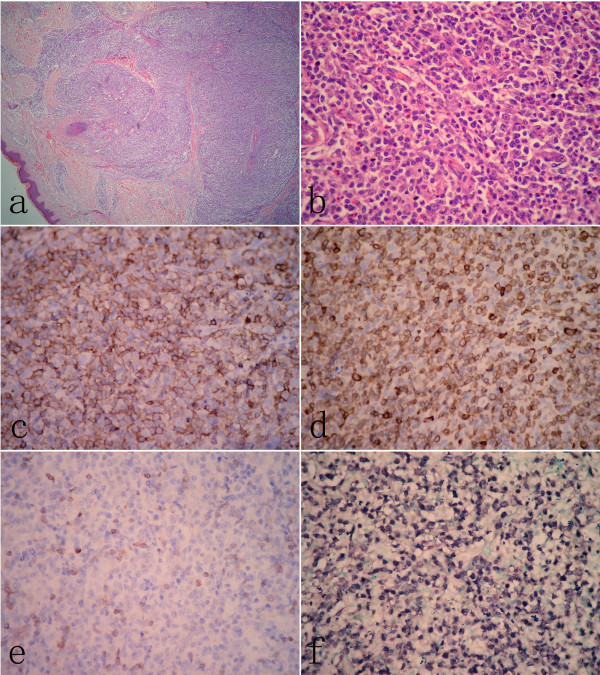
Only a few cases of extranodal Epstein-Barr virus (EBV)-associated B-cell lymphomas arising from patients with angioimmunoblastic T-cell lymphoma (AITL) have been described. We report a case of AITL of which secondary cutaneous EBV-associated diffuse large B-cell lymphoma (DLBCL) developed after the initial diagnosis of AITL. A 65-year-old Chinese male patient was diagnosed as AITL based on typical histological and immunohistochemical characteristics in biopsy of the enlarged right inguinal lymph nodes. The patient initially received 6 cycles of chemotherapy with CHOP regimen (cyclophosphamide, vincristine, adriamycin, prednisone), but his symptoms did not disappear. Nineteen months after initial diagnosis of AITL, the patient was hospitalized again because of multiple plaques and nodules on the skin. The skin biopsy was performed, but this time the tumor was composed of large, polymorphous population of lymphocytes with CD20 and CD79a positive on immunohistochemical staining. The tumor cells were strong positive for EBER by in situ hybridization. The findings of skin biopsy were compatible with EBV-associated DLBCL. CHOP-R chemotherapy (cyclophosphamide, doxorubicin, vincristine, prednisone and rituximab) was then administered, resulting in partial response of the disease with pancytopenia and suppression of cellular immunity. To our knowledge, this is the first case of cutaneous EBV-associated DLBCL originated from AITL in Chinese pepole. We suggest the patients with AITL should perform lymph node and skin biopsies regularly in the course of the disease to detect the progression of secondary lymphomas.
Figures
Similar articles
-
Diffuse large B-cell lymphoma in patient after treatment of angioimmunoblastic T-cell lymphoma.Coll Antropol. 2010 Mar;34(1):241-5. Coll Antropol. 2010. PMID: 20432757
-
Epstein-Barr Virus-Induced Cutaneous Diffuse Large B-Cell Lymphoma in a Patient With Angioimmunoblastic T-Cell Lymphoma.Am J Dermatopathol. 2019 Dec;41(12):927-930. doi: 10.1097/DAD.0000000000001371. Am J Dermatopathol. 2019. PMID: 31599749
-
Secondary Cutaneous Epstein-Barr Virus-associated Diffuse Large B-cell Lymphoma with Hodgkin/Reed-Sternberg-like Cells in a Patient with Angioimmunoblastic T-cell Lymphoma.Acta Derm Venereol. 2018 Nov 5;98(10):981-982. doi: 10.2340/00015555-2996. Acta Derm Venereol. 2018. PMID: 29956714 No abstract available.
-
Composite B-cell and T-cell lymphomas: clinical, pathological, and molecular features of three cases and literature review.J Zhejiang Univ Sci B. 2023 Aug 15;24(8):711-722. doi: 10.1631/jzus.B2300181. J Zhejiang Univ Sci B. 2023. PMID: 37551557 Free PMC article. Review.
-
Endoscopic appearance of AIDS-related gastrointestinal lymphoma with c-MYC rearrangements: case report and literature review.World J Gastroenterol. 2013 Aug 7;19(29):4827-31. doi: 10.3748/wjg.v19.i29.4827. World J Gastroenterol. 2013. PMID: 23922484 Free PMC article. Review.
Cited by
-
Discordant mycosis fungoides and cutaneous B-cell lymphoma: A case report and review of the literature.JAAD Case Rep. 2015 Jun 17;1(4):219-21. doi: 10.1016/j.jdcr.2015.04.015. eCollection 2015 Jul. JAAD Case Rep. 2015. PMID: 27051734 Free PMC article. No abstract available.
-
Specific Soft-Tissue Invasion and LMP1 Expression Are Potential Indicators of Extranodal NK/T Cell Lymphoma, Nasal Type.Med Sci Monit. 2018 Oct 25;24:7603-7613. doi: 10.12659/MSM.909152. Med Sci Monit. 2018. PMID: 30356034 Free PMC article.
-
Epstein-Barr virus positive diffuse large B-cell lymphoma transformed into angioimmunoblastic T-cell lymphoma after treatment.Clin Case Rep. 2021 May 5;9(5):e04083. doi: 10.1002/ccr3.4083. eCollection 2021 May. Clin Case Rep. 2021. PMID: 34084501 Free PMC article.
-
Angioimmunoblastic T-cell lymphoma: a diagnostic challenge.Case Rep Dermatol. 2014 Dec 17;6(3):291-5. doi: 10.1159/000370302. eCollection 2014 Sep-Dec. Case Rep Dermatol. 2014. PMID: 25685133 Free PMC article.
-
Two cases of EBV infection preceding lymphoma.J Cancer Res Clin Oncol. 2022 Oct;148(10):2929-2932. doi: 10.1007/s00432-022-04145-4. Epub 2022 Jun 22. J Cancer Res Clin Oncol. 2022. PMID: 35732965 Free PMC article.
References
-
- Rüdiger T, Weisenburger DD, Anderson JR, Armitage JO, Diebold J, MacLennan KA, Nathwani BN, Ullrich F, Müller-Hermelink HK. Non-Hodgkin's Lymphoma Classification Project. Peripheral T-cell lymphoma (excluding anaplastic large-cell lymphoma): results from the Non-Hodgkin's Lymphoma Classification Project. Ann Oncol. 2002;13:140–149. doi: 10.1093/annonc/mdf033. - DOI - PubMed
-
- Dogan A, Gaulard P, Jaffe ES, Ralfkiaer E, Müller-Hermelink HK. In: WHO classification of tumours of haematopoietic and lymphoid tissues. 4. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, editor. Lyon: IARC; 2008. Angioimmunoblastic T-cell lymphoma; pp. 309–311.
-
- Abruzzo LV, Schmidt K, Weiss LM, Jaffe ES, Medeiros LJ, Sander CA, Raffeld M. B-cell lymphoma after angioimmunoblastic lymphadenopathy: a case with oligoclonal gene rearrangements associated with Epstein-Barr virus. Blood. 1993;82:241–246. - PubMed
-
- Park S, Noguera ME, Brière J, Feuillard J, Cayuela JM, Sigaux F, Brice P. Successful rituximab treatment of an EBV-related lymphoproliferative disease arising after autologous transplantation for angioimmunoblastic T-cell lymphoma. Hematol J. 2002;3:317–720. doi: 10.1038/sj.thj.6200202. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
