

Skin effector memory T cells do not recirculate and provide immune protection in alemtuzumab-treated CTCL patients
- PMID: 22261031
- PMCID: PMC3373186
- DOI: 10.1126/scitranslmed.3003008
Skin effector memory T cells do not recirculate and provide immune protection in alemtuzumab-treated CTCL patients
Abstract
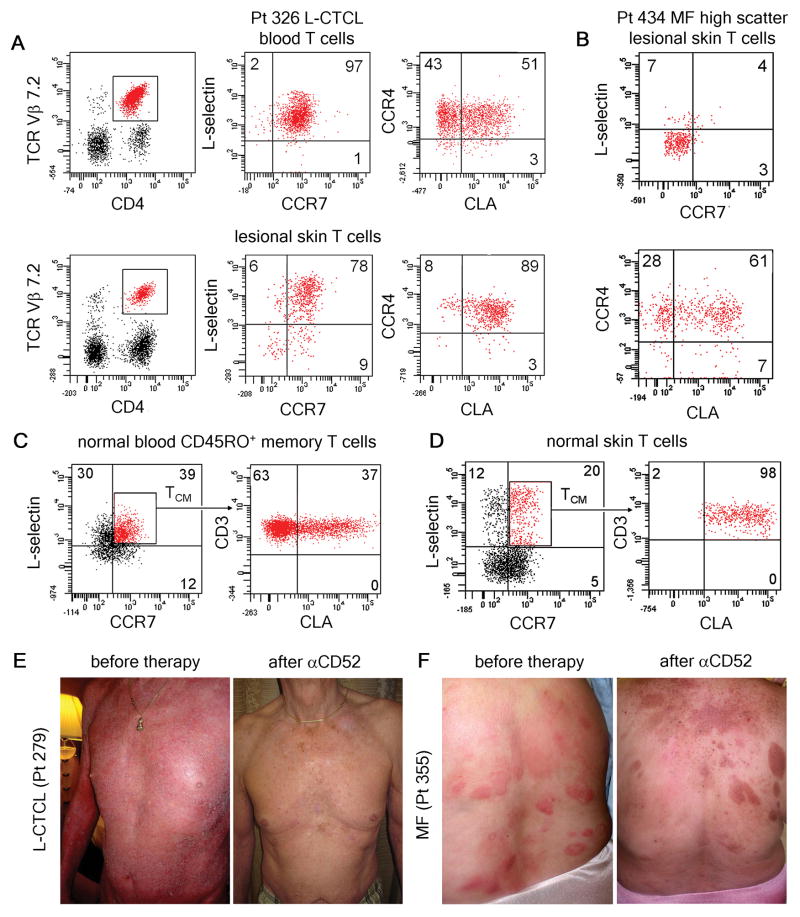
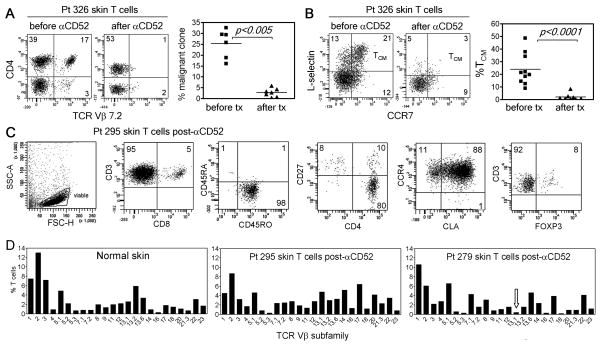
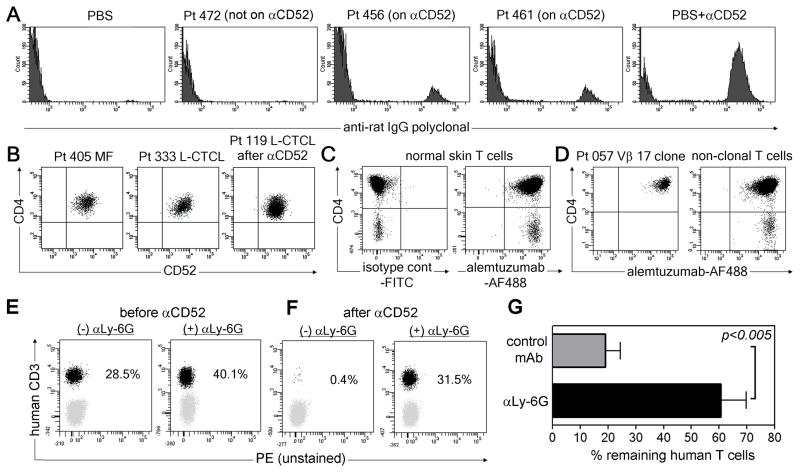
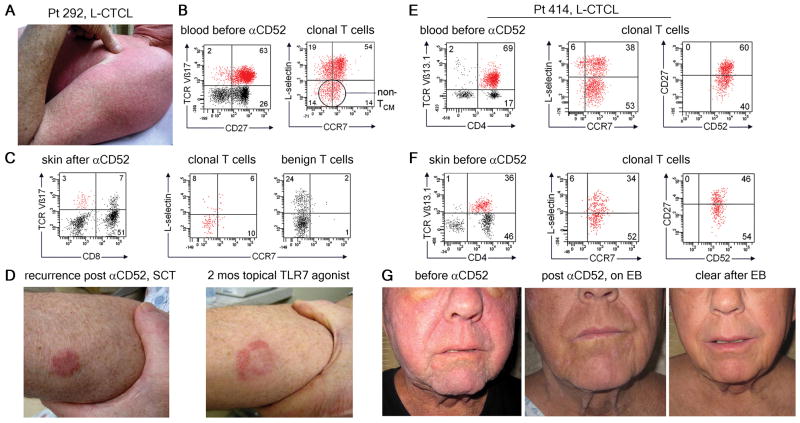
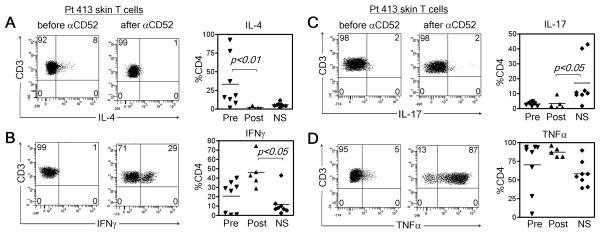
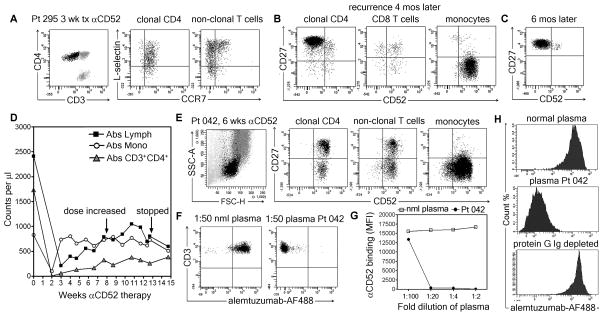
Cutaneous T cell lymphoma (CTCL) is a cancer of skin-homing T cells with variants that include leukemic CTCL (L-CTCL), a malignancy of central memory T cells (T(CM)), and mycosis fungoides (MF), a malignancy of skin resident effector memory T cells (T(EM)). We report that low-dose alemtuzumab (αCD52) effectively treated patients with refractory L-CTCL but not MF. Alemtuzumab depleted all T cells in blood and depleted both benign and malignant T(CM) from skin, but a diverse population of skin resident T(EM) remained in skin after therapy. T cell depletion with alemtuzumab required the presence of neutrophils, a cell type frequent in blood but rare in normal skin. These data suggest that T(CM) were depleted because they recirculate between the blood and the skin, whereas skin resident T(EM) were spared because they are sessile and non-recirculating. After alemtuzumab treatment, skin T cells produced lower amounts of interleukin-4 and higher amounts of interferon-γ. Moreover, there was a marked lack of infections in alemtuzumab-treated L-CTCL patients despite the complete absence of T cells in the blood, suggesting that skin resident T(EM) can protect the skin from pathogens even in the absence of T cell recruitment from the circulation. Together, these data suggest that alemtuzumab may treat refractory L-CTCL without severely compromising the immune response to infection by depleting circulating T(CM) but sparing the skin resident T(EM) that provide local immune protection of the skin.
Conflict of interest statement
Figures
Comment in
-
T cell memory: Skin-deep memory.Nat Rev Immunol. 2012 Mar 22;12(4):230-1. doi: 10.1038/nri3201. Nat Rev Immunol. 2012. PMID: 22437929 No abstract available.
References
-
- Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E, Swerdlow SH, Ralfkiaer E, Chimenti S, Diaz-Perez JL, Duncan LM, Grange F, Harris NL, Kempf W, Kerl H, Kurrer M, Knobler R, Pimpinelli N, Sander C, Santucci M, Sterry W, Vermeer MH, Wechsler J, Whittaker S, Meijer CJLM. WHO-EORTC classification for cutaneous lymphomas 10.1182/blood-2004-09-3502. Blood. 2005;105:3768. - PubMed
-
- Kim YH, Liu HL, Mraz-Gernhard S, Varghese A, Hoppe RT. Long-term outcome of 525 patients with mycosis fungoides and Sezary syndrome: clinical prognostic factors and risk for disease progression. Archives of dermatology. 2003;139:857. - PubMed
-
-
NCCN Clinical Practice Guidelines in Oncology™ Non-Hodgkin’s Lymphomas Version 3.2009 Vol. 2009 To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org. (© 2009 National Comprehensive Cancer Network, Inc., 2009)..
-
-
- van Doorn R, van Kester MS, Dijkman R, Vermeer MH, Mulder AA, Szuhai K, Knijnenburg J, Boer JM, Willemze R, Tensen CP. Oncogenomic analysis of mycosis fungoides reveals major differences with Sezary syndrome. Blood. 2009;113:127. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
