

Angiogenic factors and the risk of adverse outcomes in women with suspected preeclampsia
- PMID: 22261192
- PMCID: PMC3319742
- DOI: 10.1161/CIRCULATIONAHA.111.054361
Angiogenic factors and the risk of adverse outcomes in women with suspected preeclampsia
Abstract
Background: An imbalance in circulating angiogenic factors plays a central role in the pathogenesis of preeclampsia.
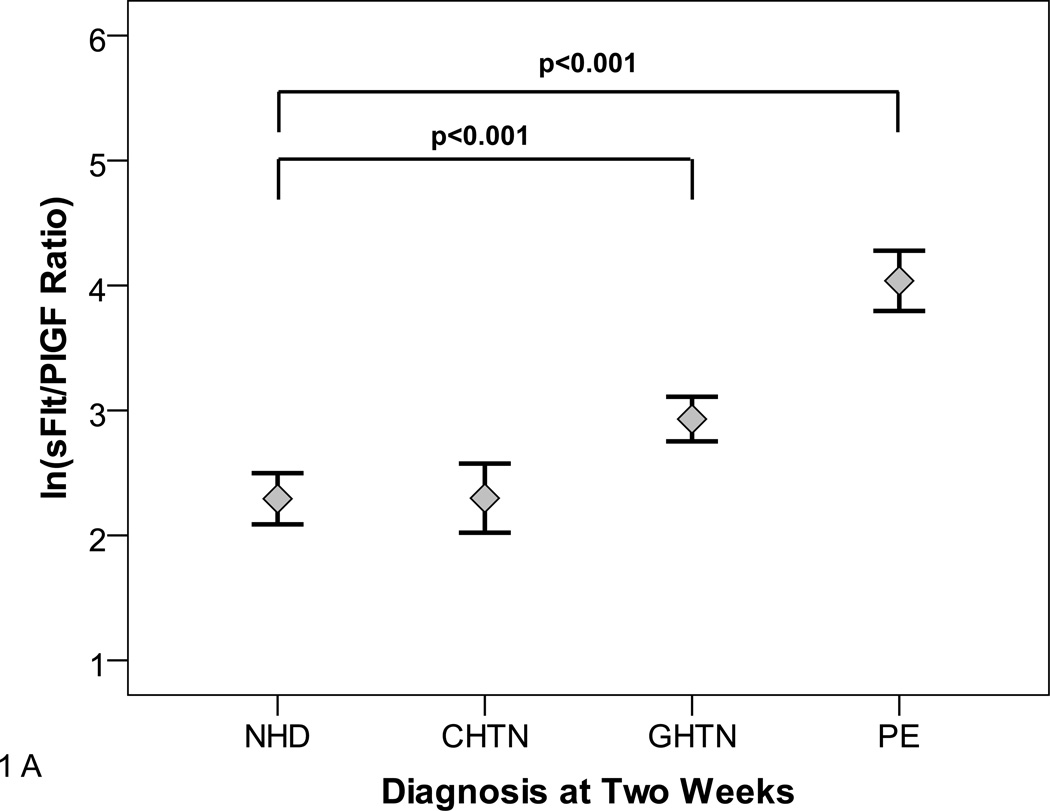
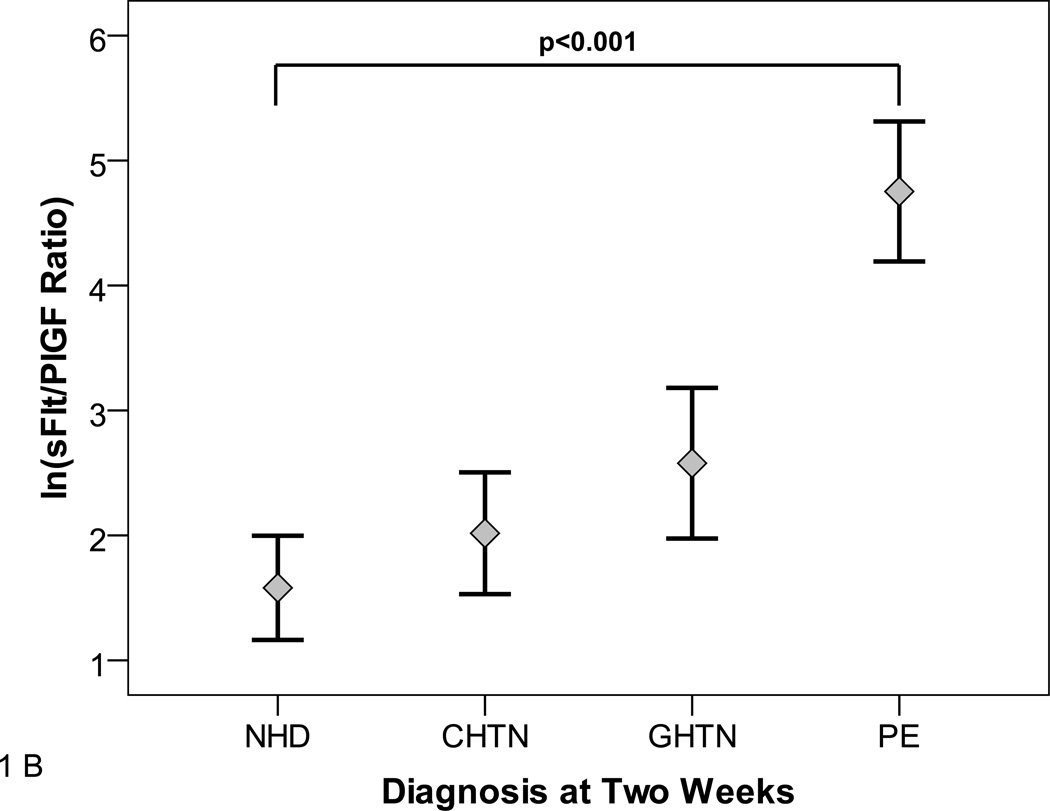
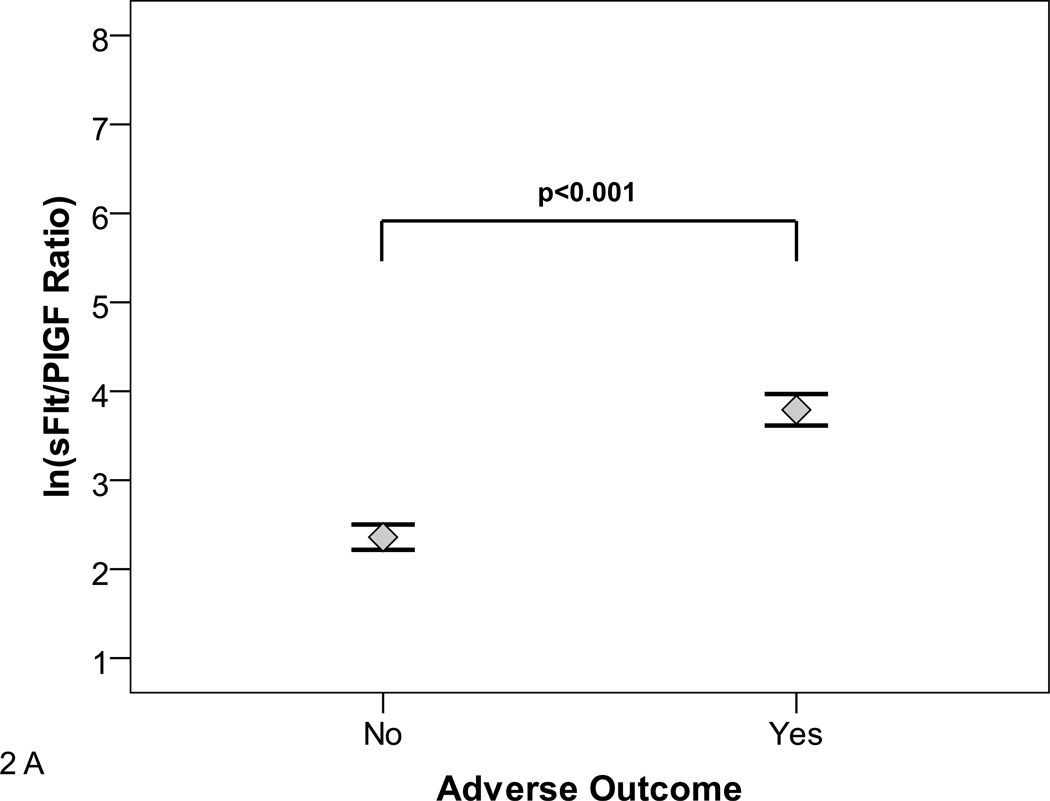
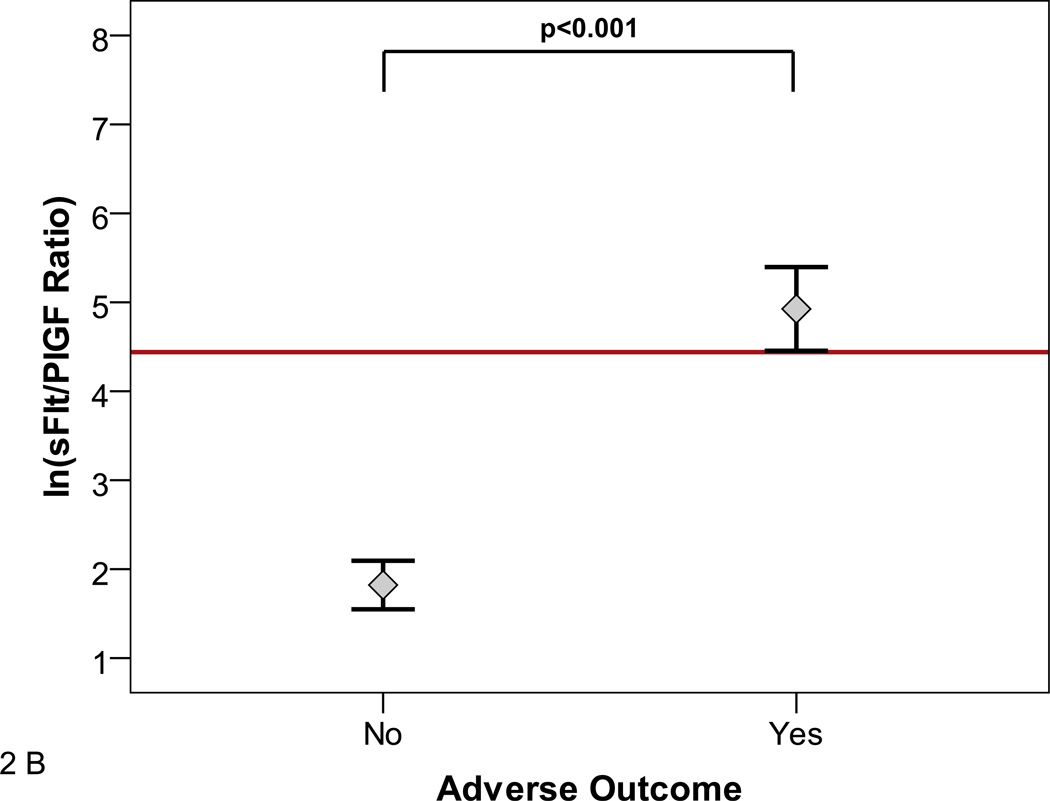
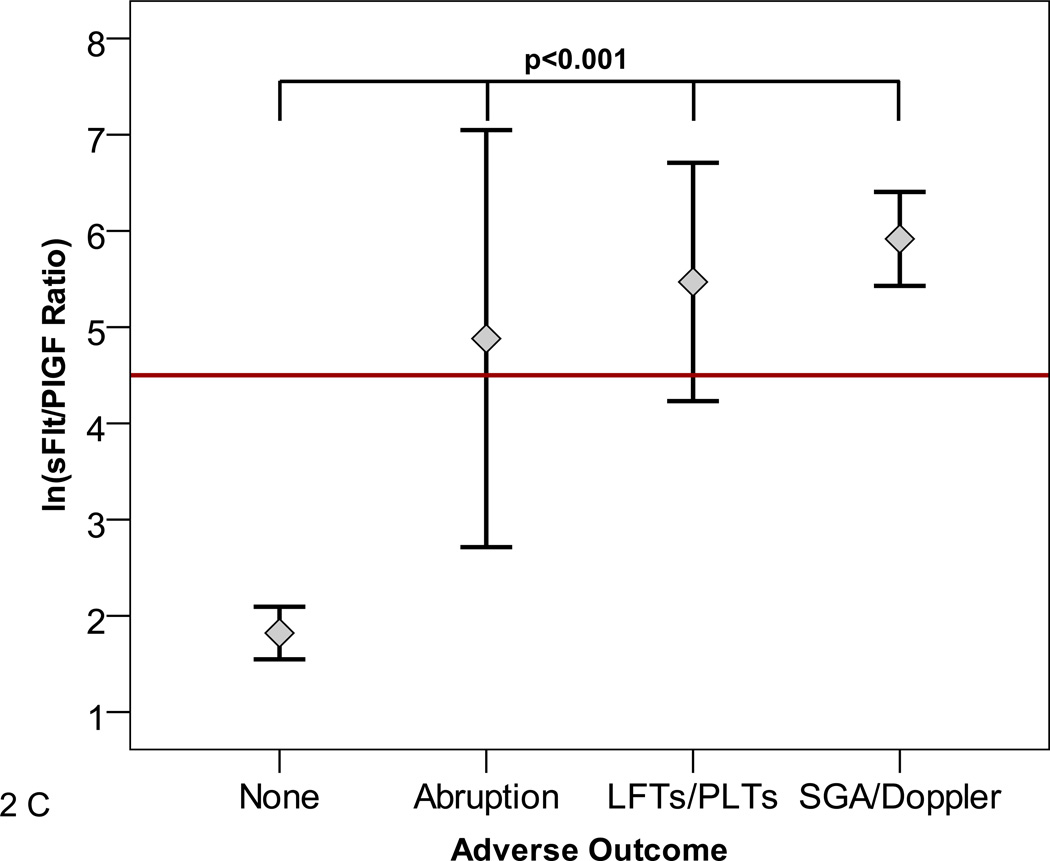
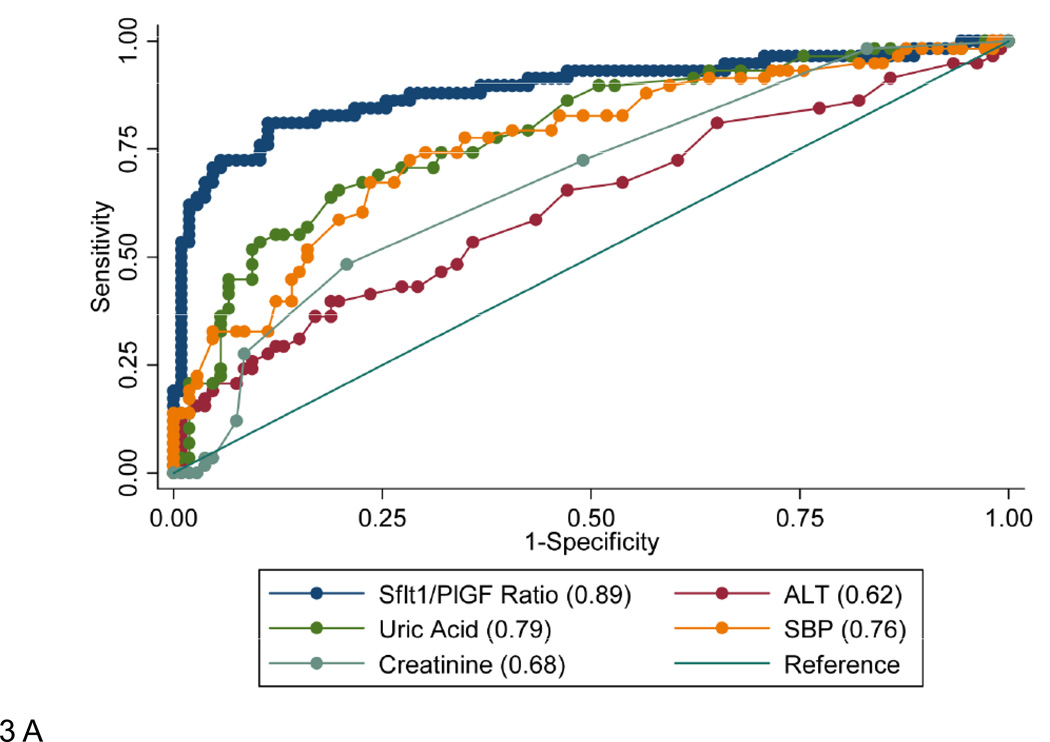
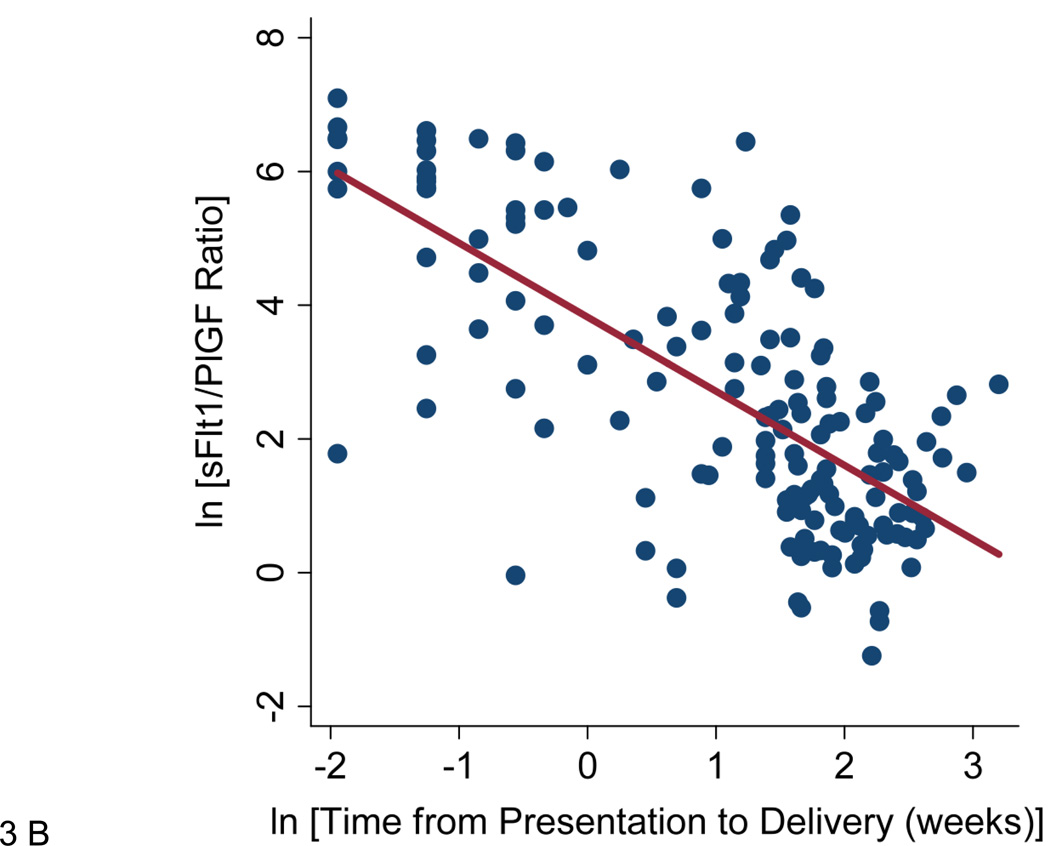
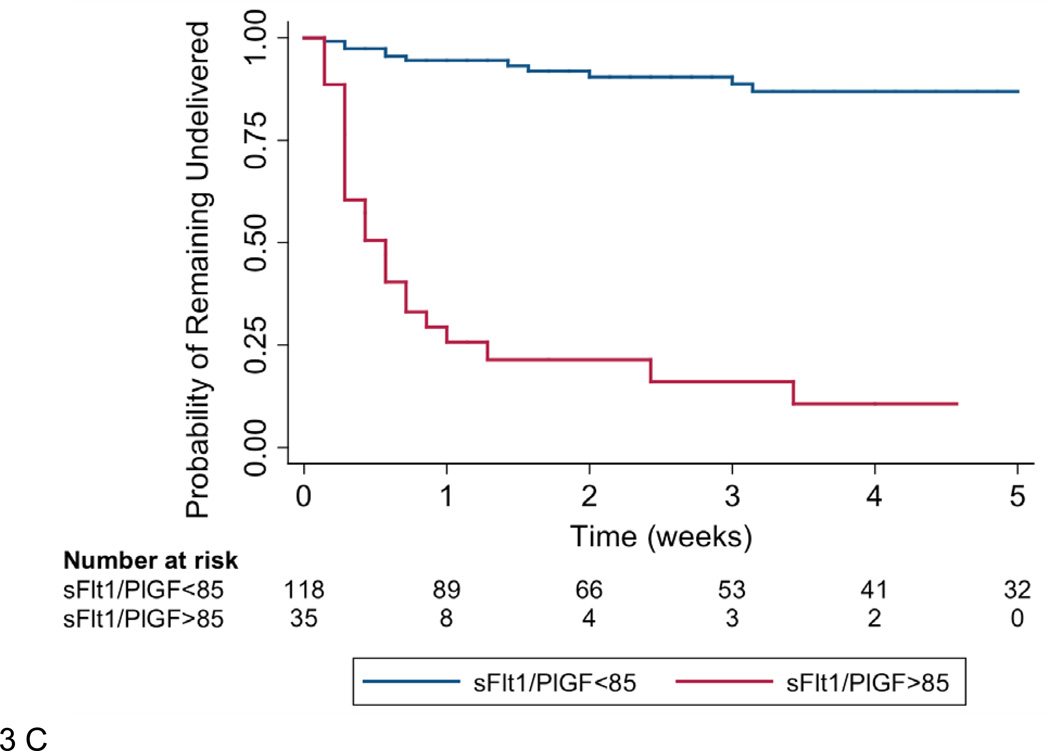
Methods and results: We prospectively studied 616 women who were evaluated for suspected preeclampsia. We measured plasma levels of antiangiogenic soluble fms-like tyrosine kinase 1 (sFlt1) and proangiogenic placental growth factor (PlGF) at presentation and examined for an association between the sFlt1/PlGF ratio and subsequent adverse maternal and perinatal outcomes within 2 weeks. The median sFlt1/PlGF ratio at presentation was elevated in participants who experienced any adverse outcome compared with those who did not (47.0 [25th-75th percentile, 15.5-112.2] versus 10.8 [25th-75th percentile, 4.1-28.6]; P<0.0001). Among those presenting at <34 weeks (n=167), the results were more striking (226.6 [25th-75th percentile, 50.4-547.3] versus 4.5 [25th-75th percentile, 2.0-13.5]; P<0.0001), and the risk was markedly elevated when the highest sFlt1/PlGF ratio tertile was compared with the lowest (odds ratio, 47.8; 95% confidence interval, 14.6-156.6). Among participants presenting at <34 weeks, the addition of sFlt1/PlGF ratio to hypertension and proteinuria significantly improved the prediction for subsequent adverse outcomes (area under the curve, 0.93 for hypertension, proteinuria, and sFlt1/PlGF versus 0.84 for hypertension and proteinuria alone; P=0.001). Delivery occurred within 2 weeks of presentation in 86.0% of women with an sFlt1/PlGF ratio ≥85 compared with 15.8% of women with an sFlt1/PlGF ratio <85 (hazard ratio, 15.2; 95% confidence interval, 8.0-28.7).
Conclusions: In women with suspected preeclampsia presenting at <34 weeks, circulating sFlt1/PlGF ratio predicts adverse outcomes occurring within 2 weeks. The accuracy of this test is substantially better than that of current approaches and may be useful in risk stratification and management. Additional studies are warranted to validate these findings.
Conflict of interest statement
Dr. Verlohren is a consultant to Roche Diagnostics. Dr. Thadhani is a co-inventor on patents related to the prediction of preeclampsia that has been out licensed to diagnostic companies and has financial interest in Aggamin LLC. Dr. Karumanchi is a co-inventor of multiple patents related to angiogenic proteins for the diagnosis and therapy of preeclampsia. These patents have been licensed to multiple companies. Dr. Karumanchi reports having served as a consultant to Roche and Beckman Coulter and has financial interest in Aggamin LLC. The remaining authors report no conflicts.
Figures
References
-
- Wallis AB, Saftlas AF, Hsia J, Atrash HK. Secular trends in the rates of preeclampsia, eclampsia, and gestational hypertension, united states, 1987–2004. Am J Hypertens. 2008;21:521–526. - PubMed
-
- Friedman SA, Schiff E, Kao L, Sibai BM. Neonatal outcome after preterm delivery for preeclampsia. Am J Obstet Gynecol. 1995;172:1785–1788. discussion 1788–1792. - PubMed
-
- Acog practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, january 2002. Obstet Gynecol. 2002;99:159–167. - PubMed
-
- Sibai BM, Stella CL. Diagnosis and management of atypical preeclampsia-eclampsia. Am J Obstet Gynecol. 2009;200:481, e481–e487. - PubMed
-
- Ganzevoort W, Rep A, de Vries JI, Bonsel GJ, Wolf H. Prediction of maternal complications and adverse infant outcome at admission for temporizing management of early-onset severe hypertensive disorders of pregnancy. Am J Obstet Gynecol. 2006;195:495–503. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
