

"Sweet spot" for endoleak detection: optimizing contrast to noise using low keV reconstructions from fast-switch kVp dual-energy CT
- PMID: 22261775
- PMCID: PMC3265790
- DOI: 10.1097/RCT.0b013e31824258cb
"Sweet spot" for endoleak detection: optimizing contrast to noise using low keV reconstructions from fast-switch kVp dual-energy CT
Abstract
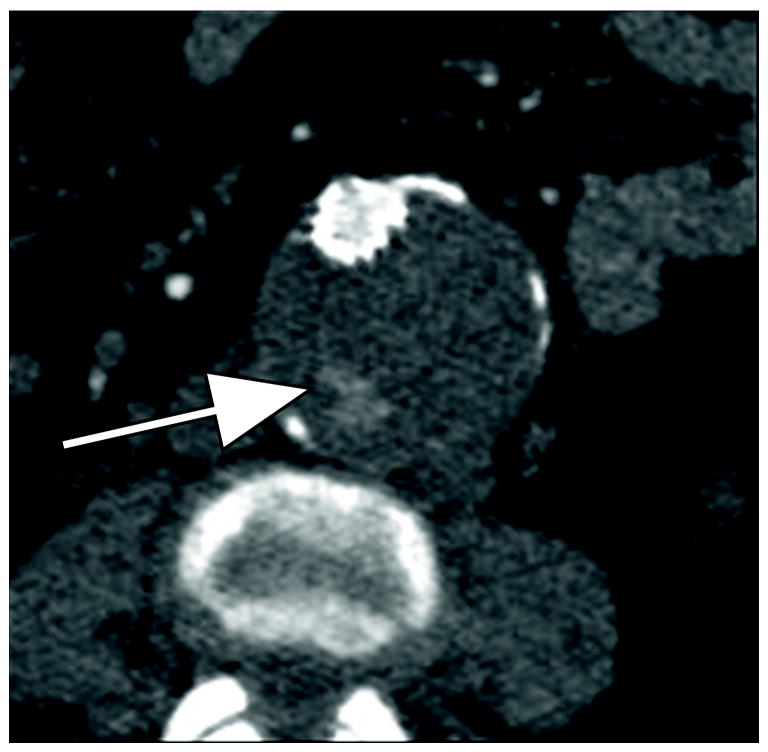
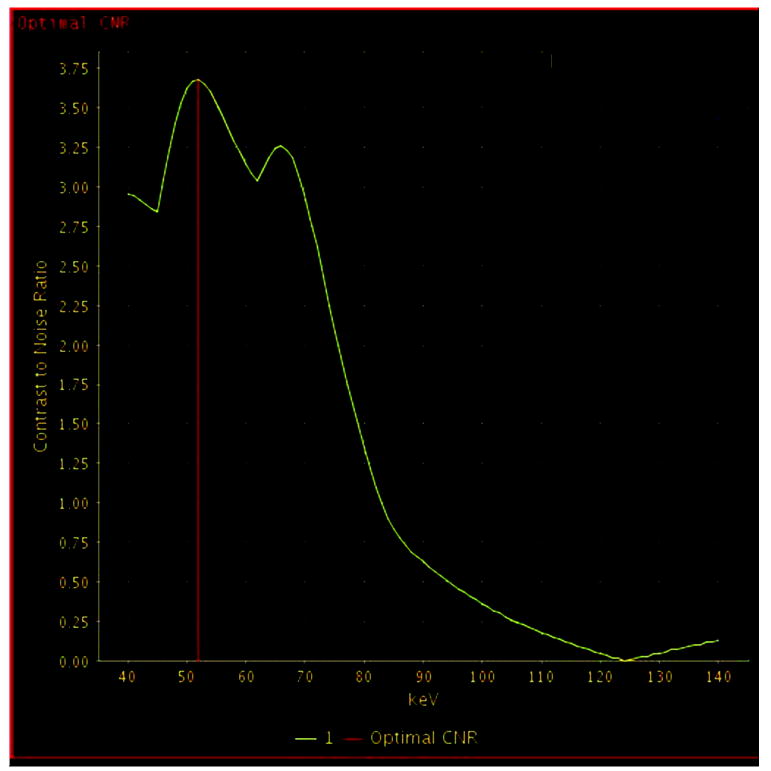
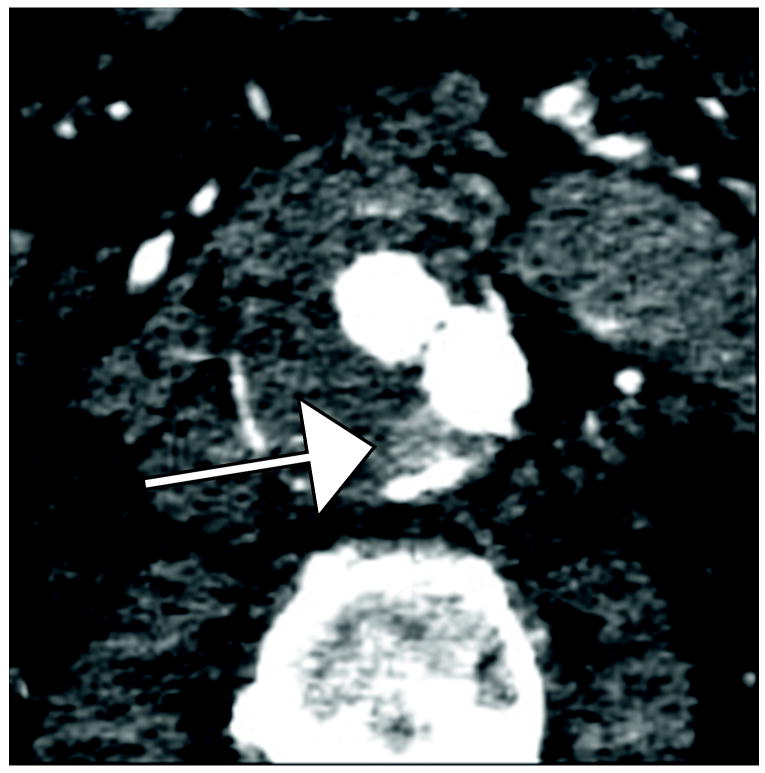
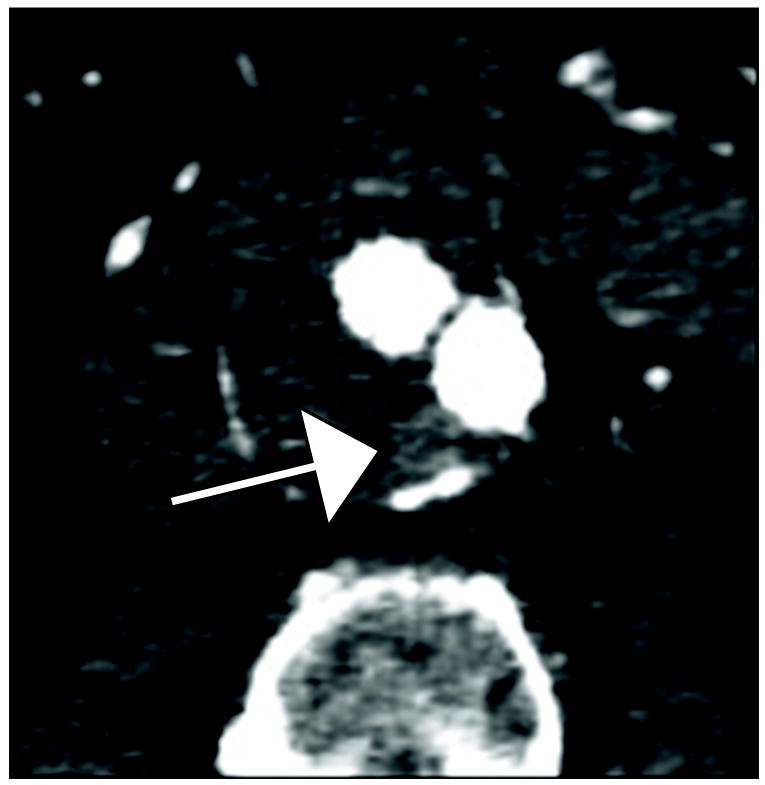
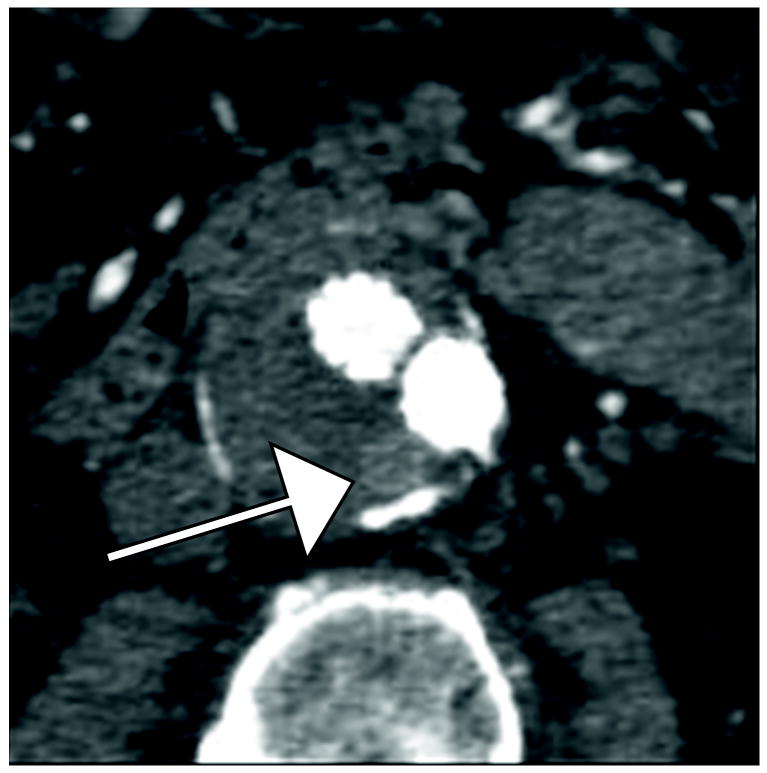
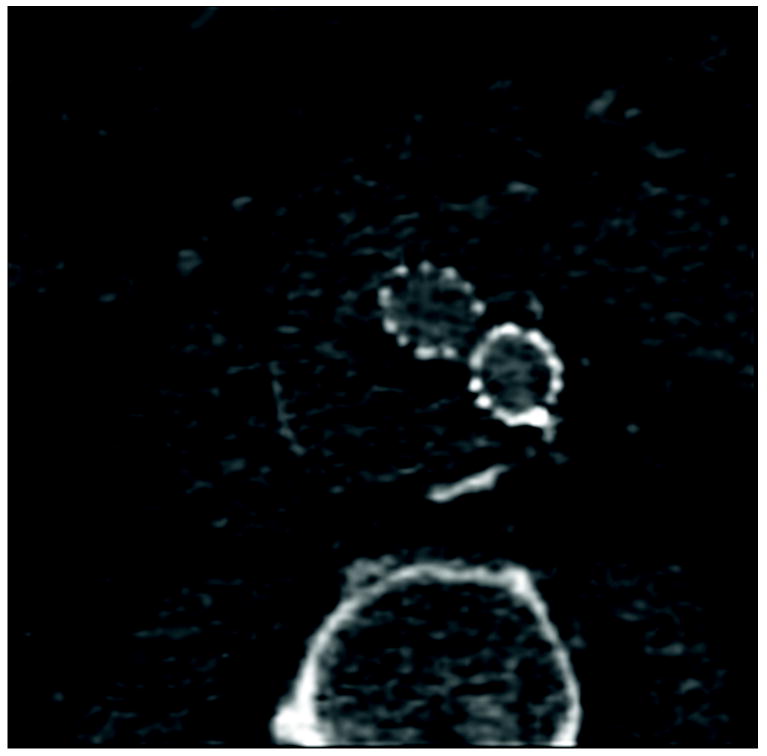
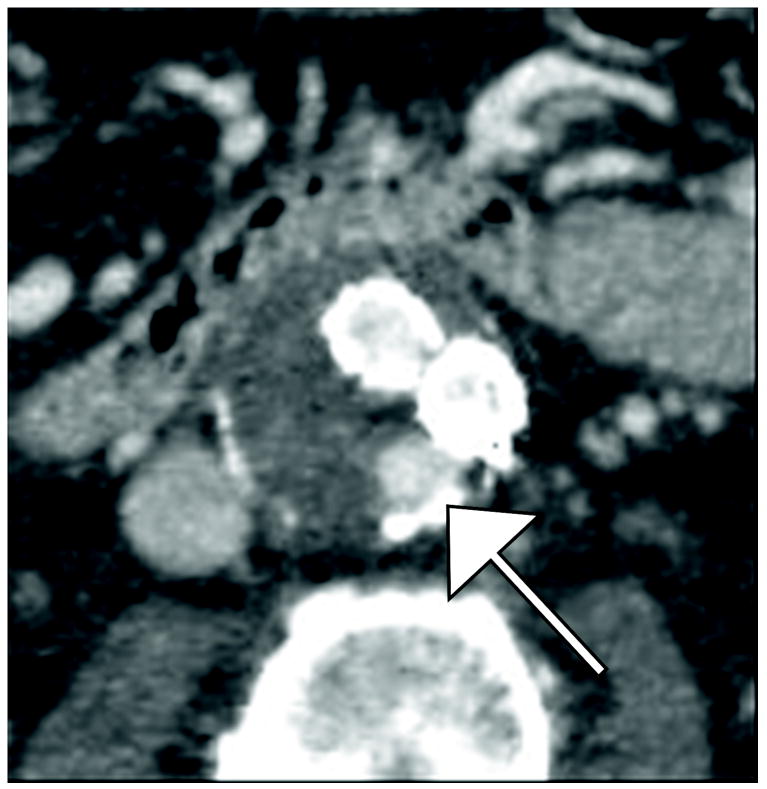
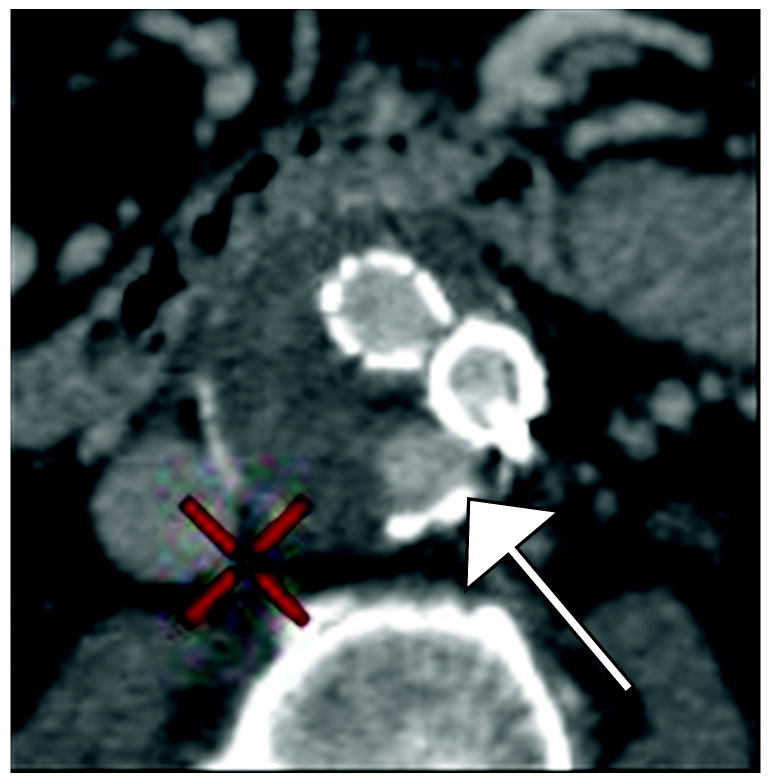
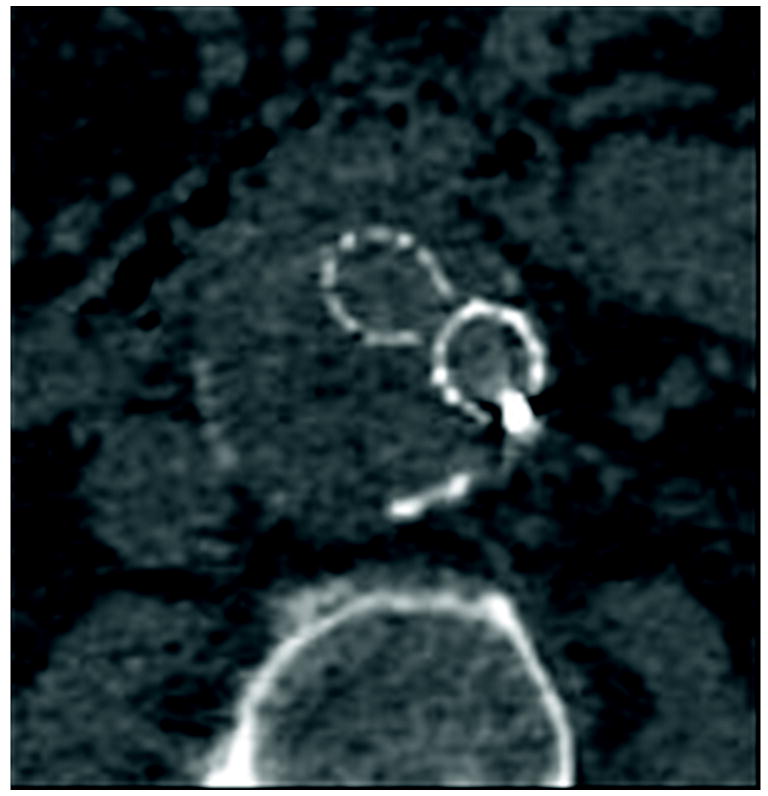
Objective: To assess endoleak detection and conspicuity using low-kiloelectron volt (keV) monochromatic reconstructions of single-source (fast-switch kilovolt [peak]) dual-energy data sets.
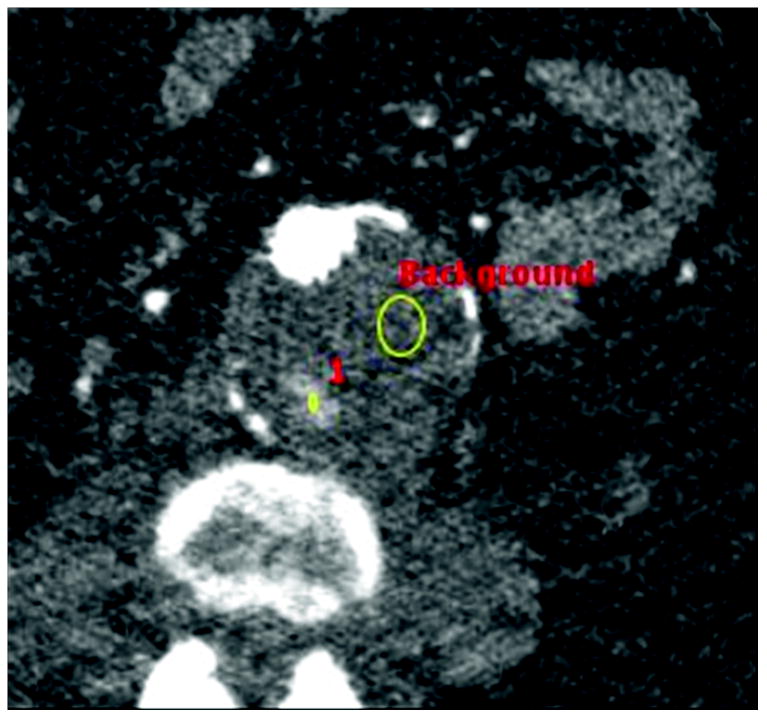
Methods: With approval of the institutional review board, multiphasic dual-energy computed tomographic (CT) scans for aortic endograft surveillance were retrospectively reviewed for 39 patients. Two abdominal radiologists each performed 2 separate reading sessions, at 55-keV and standard 75-keV reconstruction, respectively. The readers tabulated endoleak presence, conspicuity on 1-to-5 scale, and type overall and in arterial and venous phases. Originally, dictated reports in medical records were used as criterion standard.
Results: Original dictations identified 19 endoleaks (9 abdominal and 10 thoracic), 13 of which were type II. The blinded readers (R1 and R2) exhibited good to very good intraobserver and interobserver agreement. Endoleak detection was higher at 55 keV than at 75 keV (sensitivity, 100% (95% confidence interval [CI], 82.4%-100.0%) and 84.2% (95% CI, 60.4-96.6%) at 55 keV vs 79% (95% CI, 54.4-94.0%) and 68.4% (95% CI, 43.5%-87.4%) at 75 keV in venous phase). Further, endoleak conspicuity ratings (where original dictation showed positive leak) were higher at 55 keV than at 75 keV, which was a significant difference for R2 in the overall ratings (P = 0.03) and for both readers in the venous phase ratings (R1, P = 0.01; R2, P = 0.004). There was no difference in endoleak type characterization between the kiloelectron volt levels.
Conclusion: Sensitivity for endoleak detection and overall endoleak conspicuity ratings were both higher at 55 keV than 75 keV, favoring the inclusion of a lower-energy monochromatic reconstruction for endoleak surveillance protocols with dual-energy computed tomography.
Figures

Similar articles
-
Multi-Energy Low-Kiloelectron Volt versus Single-Energy Low-Kilovolt Images for Endoleak Detection at CT Angiography of the Aorta.Radiol Cardiothorac Imaging. 2024 Apr;6(2):e230217. doi: 10.1148/ryct.230217. Radiol Cardiothorac Imaging. 2024. PMID: 38451189 Free PMC article. Clinical Trial.
-
Aortic endograft surveillance: use of fast-switch kVp dual-energy computed tomography with virtual noncontrast imaging.J Comput Assist Tomogr. 2011 Nov-Dec;35(6):742-6. doi: 10.1097/RCT.0b013e3182372c14. J Comput Assist Tomogr. 2011. PMID: 22082546
-
Indirect computed tomography venography of the lower extremities using single-source dual-energy computed tomography: advantage of low-kiloelectron volt monochromatic images.J Vasc Interv Radiol. 2012 Jul;23(7):879-86. doi: 10.1016/j.jvir.2012.04.012. Epub 2012 May 24. J Vasc Interv Radiol. 2012. PMID: 22633619
-
Enhanced visualization in endoleak detection through iterative and AI-noise optimized spectral reconstructions.Sci Rep. 2024 Feb 15;14(1):3845. doi: 10.1038/s41598-024-54502-1. Sci Rep. 2024. PMID: 38360941 Free PMC article.
-
Dual-energy liver CT: effect of monochromatic imaging on lesion detection, conspicuity, and contrast-to-noise ratio of hypervascular lesions on late arterial phase.AJR Am J Roentgenol. 2014 Sep;203(3):601-6. doi: 10.2214/AJR.13.11337. AJR Am J Roentgenol. 2014. PMID: 25148163
Cited by
-
The value of metal artifact reduction and iterative algorithms in dual energy CT angiography in patients after complex endovascular aortic aneurysm repair.Heliyon. 2023 Oct 12;9(10):e20700. doi: 10.1016/j.heliyon.2023.e20700. eCollection 2023 Oct. Heliyon. 2023. PMID: 37876478 Free PMC article.
-
Dual Energy CT Angiography of Peripheral Arterial Disease: Feasibility of Using Lower Contrast Medium Volume.PLoS One. 2015 Sep 29;10(9):e0139275. doi: 10.1371/journal.pone.0139275. eCollection 2015. PLoS One. 2015. PMID: 26418007 Free PMC article. Clinical Trial.
-
Advanced image-based virtual monoenergetic dual-energy CT angiography of the abdomen: optimization of kiloelectron volt settings to improve image contrast.Eur Radiol. 2016 Jun;26(6):1863-70. doi: 10.1007/s00330-015-3970-2. Epub 2015 Sep 3. Eur Radiol. 2016. PMID: 26334508
-
Dual-Energy CT: New Horizon in Medical Imaging.Korean J Radiol. 2017 Jul-Aug;18(4):555-569. doi: 10.3348/kjr.2017.18.4.555. Epub 2017 May 19. Korean J Radiol. 2017. PMID: 28670151 Free PMC article. Review.
-
Assessing the diagnostic accuracy of artificial intelligence in post-endovascular aneurysm repair endoleak detection using dual-energy computed tomography angiography.Pol J Radiol. 2024 Aug 28;89:e420-e427. doi: 10.5114/pjr/192115. eCollection 2024. Pol J Radiol. 2024. PMID: 39257927 Free PMC article.
References
-
- Prinssen M, Wixon CL, Buskens E, et al. Surveillance after endovascular aneurysm repair: diagnostics, complications, and associated costs. Ann Vasc Surg. 2004;18:421–7. - PubMed
-
- Black SA, Carrell TWG, Bell RE, et al. Long-term surveillance with computed tomography after endovascular aneurysm repair may not be justified. British journal of surgery. 2009;96:1280–1283. - PubMed
-
- Bley T, Chase P, Reeder S, et al. Endovascular abdominal aortic aneurysm repair: nonenhanced volumetric CT for follow-up. Radiology. 2009;253:253–262. - PubMed
-
- Wieners G, Meyer F, Halloul Z, et al. Detection of type II endoleak after endovascular aortic repair: comparison between magnetic resonance angiography and blood-pool contrast agent and dual-phase computed tomography angiography. Cardiovascular and interventional radiology. 2010;33:1135–1142. - PubMed
-
- Chaer R, Gushchin A, Rhee R, et al. Duplex ultrasound as the sole long-term surveillance method post-endovascular aneurysm repair: a safe alternative for stable aneurysms. Journal of vascular surgery. 2009;49:845–9. - PubMed
