

Associations between psychiatric comorbidities and sleep disturbances in children with attention-deficit/hyperactivity disorder
- PMID: 22261833
- PMCID: PMC4078726
- DOI: 10.1097/DBP.0b013e31823f6853
Associations between psychiatric comorbidities and sleep disturbances in children with attention-deficit/hyperactivity disorder
Abstract
Objective: Children with attention-deficit/hyperactivity disorder (ADHD) often have sleep complaints and also higher rates of psychiatric comorbidities such as mood and anxiety disorders that may affect sleep. The authors hypothesized that children with ADHD and psychiatric comorbidities would have higher overall sleep disturbance scores as measured by a sleep questionnaire than children with ADHD without comorbidities.
Methods: This cross-sectional analysis in an academic center studied 317 children with ADHD; 195 subjects had no comorbid conditions, 60 were anxious and 62 were depressed. Participants completed the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present State, 4th Revised Edition and the Children's Sleep Habits Questionnaire.
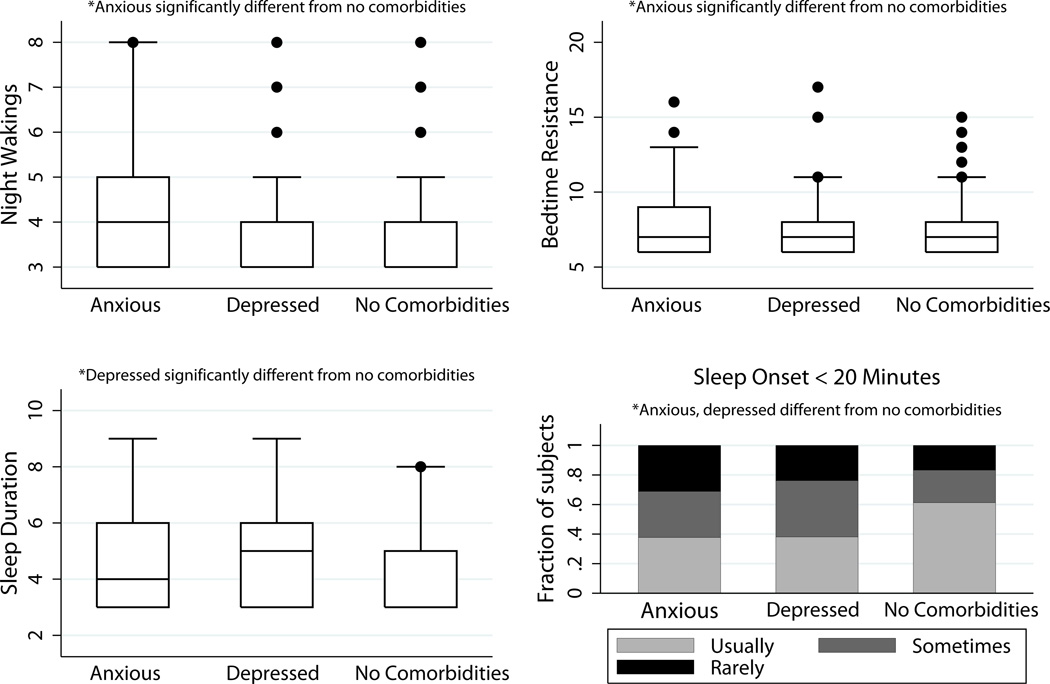
Results: Median age (range) was 8.9 (6-18.7) years; 78% were male. Median (interquartile range) Total Sleep Disturbance Score (TSDS) on Children's Sleep Habits Questionnaire for subjects with no comorbidities was 44 (40-49); anxiety, 48 (43-54); and depression, 46 (41-52). Compared with subjects without comorbidities, TSDS in anxious subjects was greater (p = .008). TSDS in depressed subjects was not significantly different. Compared with subjects without comorbidities, anxious subjects had higher Bedtime Resistance, Sleep Onset Delay, and Night Wakings subscales (p = .03, .007, and .007, respectively); depressed subjects had higher Sleep Onset Delay and Sleep Duration subscales (p = .003 and .01, respectively).
Conclusions: Anxiety in children with ADHD contributed to higher overall sleep disturbance scores, compared with children with ADHD alone. Both comorbidities were associated with higher Sleep Onset Latency subscale scores. Further study of the impact of psychiatric comorbidities on sleep in children with ADHD is warranted.
Conflict of interest statement
The other authors have no conflicts of interest to declare.
Figures
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Washington, DC: American Psychiatric Association; 1980.
-
- Sung V, Hiscock H, Sciberras E, Efron D. Sleep problems in children with Attention-Deficit/Hyperactivity Disorder. Arch Pediatr Adolesc Med. 2008;162(4):336–342. - PubMed
-
- Ball JD, Tiernan M, Janusz J, Furr A. Sleep patterns among children with attention-deficit hyperactivity disorder: a reexamination of parent perceptions. J Pediatr Psychol. 1997;22:389–398. - PubMed
-
- Corkum P, Moldofsky H, Hogg-Johnson S, et al. Sleep problems in children with attention-deficit/hyperactivity disorder: impact of subtype, comorbidity, and stimulant medication. J Am Acad Child Adolesc Psychiatry. 1999;38(10):1285–1293. - PubMed
-
- Wiggs L, Montgomery P, Stores G. Actigraphic and parent reports of sleep patterns and sleep disorders in children with subtypes of attention-deficit/hyperactivity disorder. Sleep. 2005;28(11):1437–1445. - PubMed
