

A systematic review of validated methods for identifying atrial fibrillation using administrative data
- PMID: 22262600
- PMCID: PMC3674852
- DOI: 10.1002/pds.2317
A systematic review of validated methods for identifying atrial fibrillation using administrative data
Abstract
Purpose: The objectives of this study were to characterize the validity of algorithms to identify AF from electronic health data through a systematic review of the literature and to identify gaps needing further research.
Methods: Two reviewers examined publications during 1997-2008 that identified patients with atrial fibrillation (AF) from electronic health data and provided validation information. We abstracted information including algorithm sensitivity, specificity, and positive predictive value (PPV).
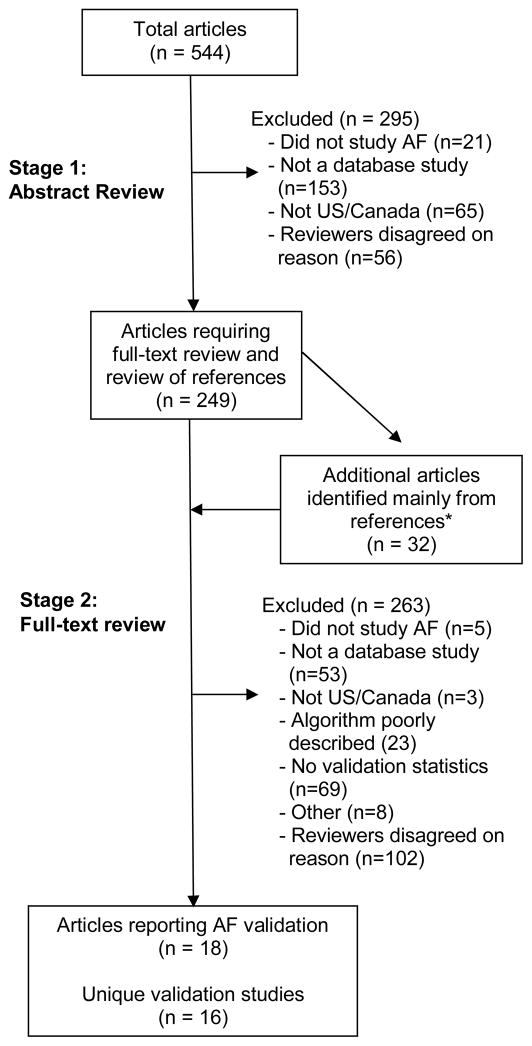
Results: We reviewed 544 abstracts and 281 full-text articles, of which 18 provided validation information from 16 unique studies. Most used data from before 2000, and 10 of 16 used only inpatient data. Three studies incorporated electronic ECG data for case identification or validation. A large proportion of prevalent AF cases identified by ICD-9 code 427.31 were valid (PPV 70%-96%, median 89%). Seven studies reported algorithm sensitivity (range, 57%-95%, median 79%). One study validated an algorithm for incident AF and reported a PPV of 77%.
Conclusions: The ICD-9 code 427.31 performed relatively well, but conclusions about algorithm validity are hindered by few recent data, use of nonrepresentative populations, and a disproportionate focus on inpatient data. An optimal contemporary algorithm would likely draw on inpatient and outpatient codes and electronic ECG data. Additional research is needed in representative, contemporary populations regarding algorithms that identify incident AF and incorporate electronic ECG data.
Copyright © 2012 John Wiley & Sons, Ltd.
Conflict of interest statement
Conflict of interests: Dr. Dublin received a Merck/American Geriatrics Society New Investigator Award. No other authors reported conflicts of interest. This manuscript was derived from a longer report which is published on the Mini-Sentinel website.
Figures
References
-
- Kannel WB, Wolf PA, Benjamin EJ, et al. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 1998;82:2N–9N. - PubMed
-
- Food and Drug Administration. Listing of DMEs is adapted from “Safety Reporting Requirements for Human Drug and Biological Products; Proposed Rule”. Department of Health and Human Services; Washington, DC: Mar 14, 2003. [accessed December 3, 2010]. http://www.fda.gov/OHRMS/DOCKETS/98fr/03-5204.pdf.
-
- The Observational Medical Outcomes Partnership (OMOP) Health Outcomes of Interest. Foundation for the National Institutes of Health; Bethesda: [accessed June 7, 2010]. http://omop.fnih.org/HOI.
-
- Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Meas. 1960;20:37–46.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
