

Laparoscopy to predict the result of primary cytoreductive surgery in advanced ovarian cancer patients (LapOvCa-trial): a multicentre randomized controlled study
- PMID: 22264278
- PMCID: PMC3292486
- DOI: 10.1186/1471-2407-12-31
Laparoscopy to predict the result of primary cytoreductive surgery in advanced ovarian cancer patients (LapOvCa-trial): a multicentre randomized controlled study
Abstract
Background: Standard treatment of advanced ovarian cancer is surgery and chemotherapy. The goal of surgery is to remove all macroscopic tumour, as the amount of residual tumour is the most important prognostic factor for survival. When removal off all tumour is considered not feasible, neoadjuvant chemotherapy (NACT) in combination with interval debulking surgery (IDS) is performed. Current methods of staging are not always accurate in predicting surgical outcome, since approximately 40% of patients will have more than 1 cm residual tumour after primary debulking surgery (PDS). In this study we aim to assess whether adding laparoscopy to the diagnostic work-up of patients suspected of advanced ovarian carcinoma may prevent unsuccessful primary debulking surgery for ovarian cancer.
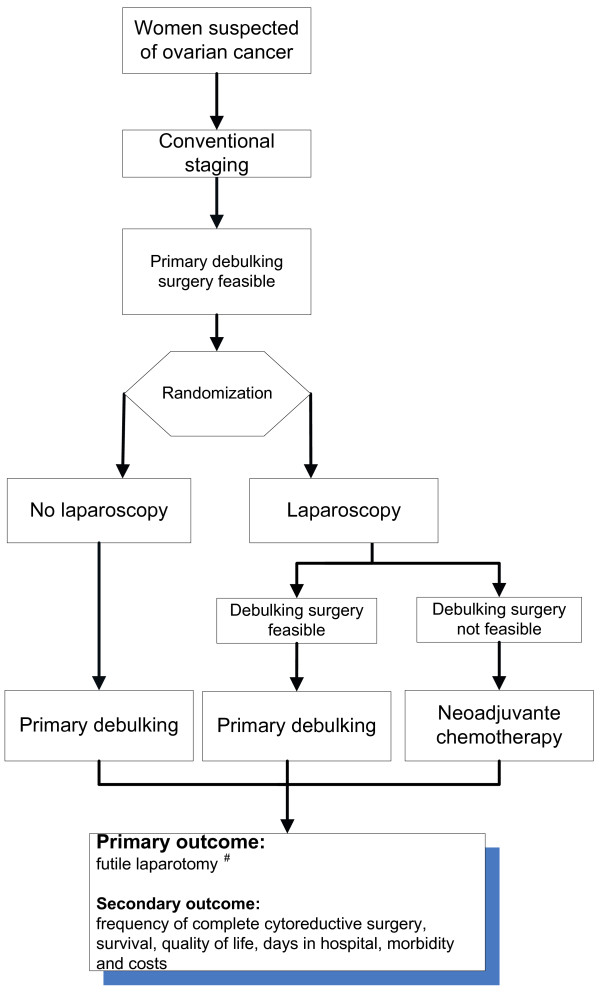
Methods: Multicentre randomized controlled trial, including all gynaecologic oncologic centres in the Netherlands and their affiliated hospitals. Patients are eligible when they are planned for PDS after conventional staging. Participants are randomized between direct PDS or additional diagnostic laparoscopy. Depending on the result of laparoscopy patients are treated by PDS within three weeks, followed by six courses of platinum based chemotherapy or with NACT and IDS 3-4 weeks after three courses of chemotherapy, followed by another three courses of chemotherapy. Primary outcome measure is the proportion of PDS's leaving more than one centimetre tumour residual in each arm. In total 200 patients will be randomized. Data will be analysed according to intention to treat.
Discussion: Patients who have disease considered to be resectable to less than one centimetre should undergo PDS to improve prognosis. However, there is a need for better diagnostic procedures because the current number of debulking surgeries leaving more than one centimetre residual tumour is still high. Laparoscopy before starting treatment for ovarian cancer can be an additional diagnostic tool to predict the outcome of PDS. Despite the absence of strong evidence and despite the possible complications, laparoscopy is already implemented in many countries. We propose a randomized multicentre trial to provide evidence on the effectiveness of laparoscopy before primary surgery for advanced stage ovarian cancer patients.
Trial registration: Netherlands Trial Register number NTR2644.
Figures
References
-
- du Bois A, Reuss A, Pujade-Lauraine E, Harter P, Ray-Coquard I, Pfisterer J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: a combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: by the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe d'Investigateurs Nationaux Pour les Etudes des Cancers de l'Ovaire (GINECO) Cancer. 2009;115:1234–1244. doi: 10.1002/cncr.24149. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
