

Injecting drug use via femoral vein puncture: preliminary findings of a point-of-care ultrasound service for opioid-dependent groin injectors in treatment
- PMID: 22264343
- PMCID: PMC3305527
- DOI: 10.1186/1477-7517-9-6
Injecting drug use via femoral vein puncture: preliminary findings of a point-of-care ultrasound service for opioid-dependent groin injectors in treatment
Abstract
Background: Within the UK, injecting in the femoral vein (FV), often called 'groin injecting', is a serious cause of risk and harm. This study aimed to use ultrasound scanning as a means to engage groin injectors (GIs), examine their femoral injecting sites and assess their venous health, with the intention of developing improved responses.
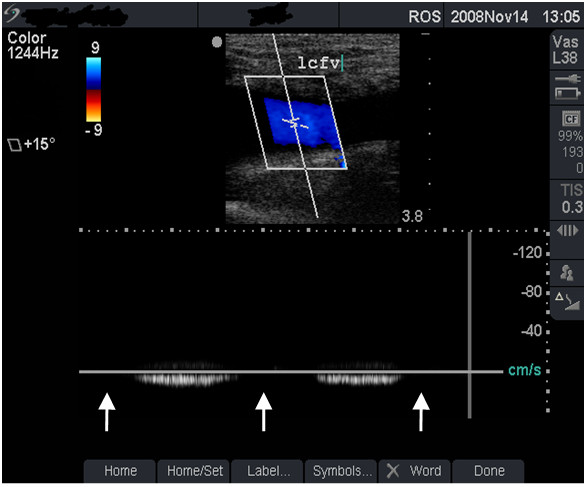
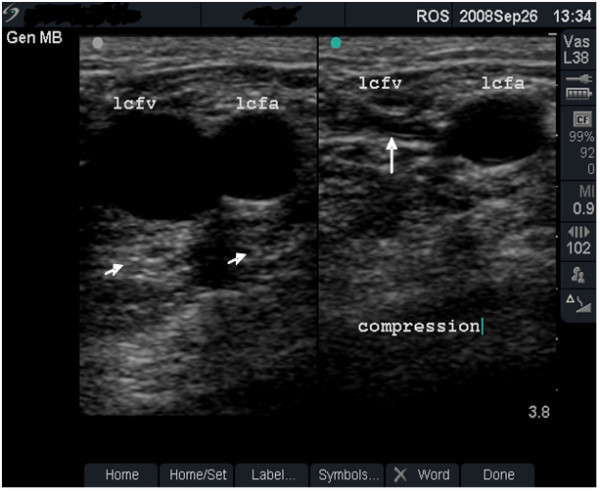
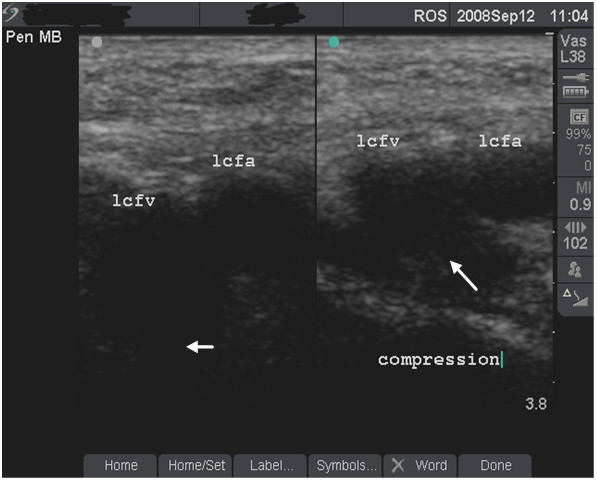
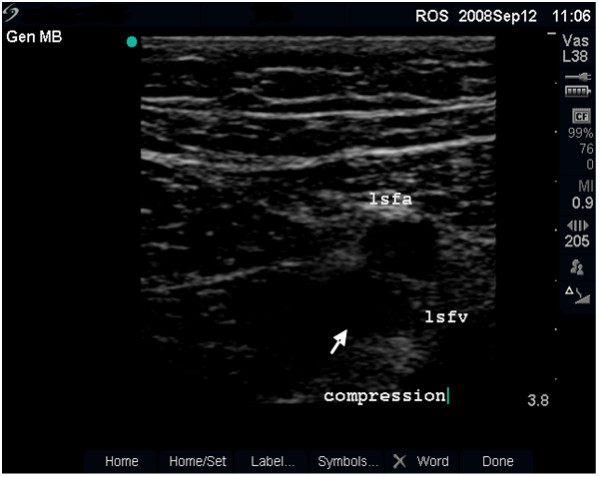
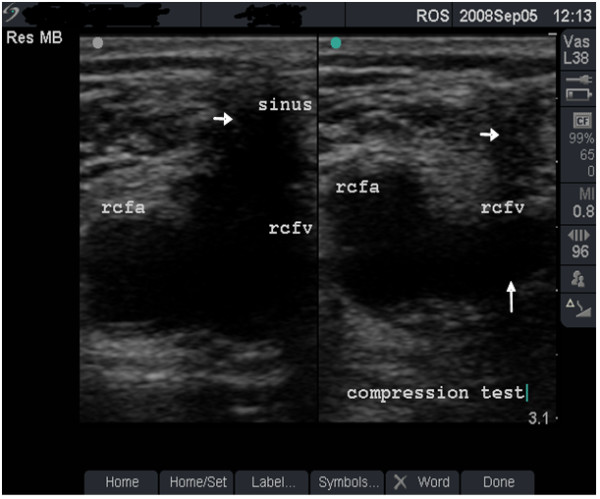
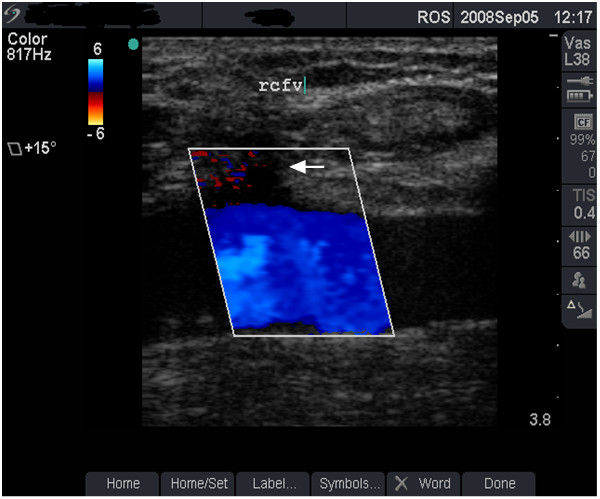
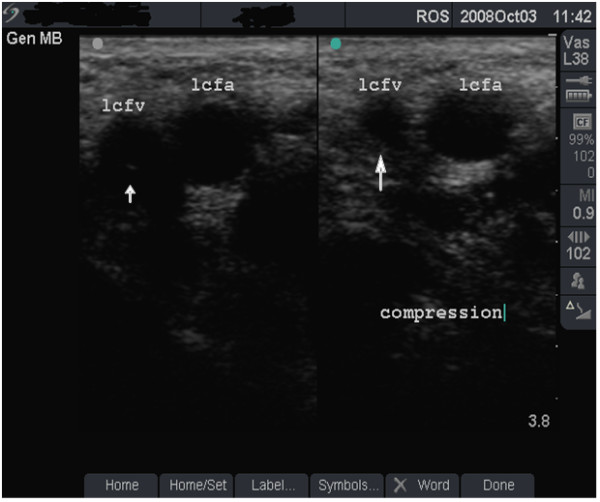
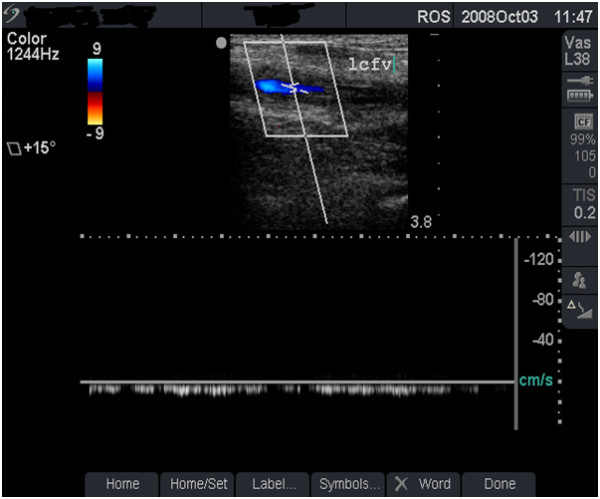
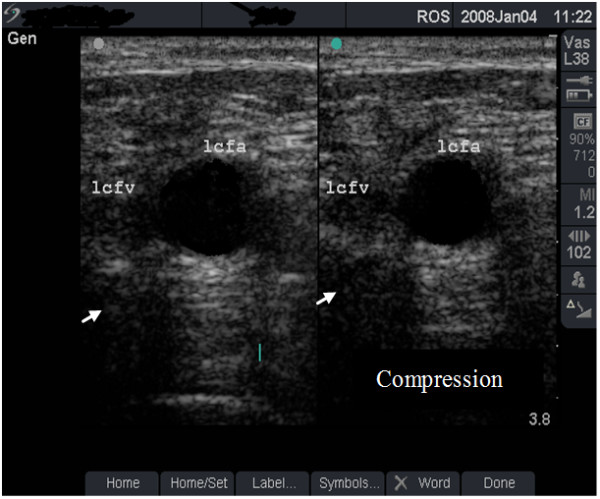
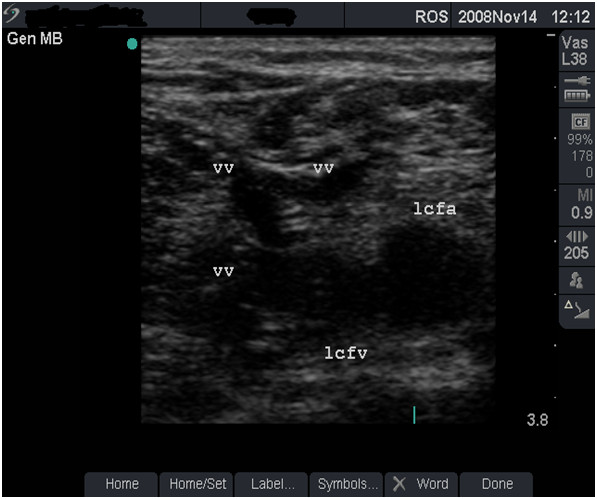
Methods: Between September 2006 and March 2009, GIs attending a network of community drug treatment centres in South East England were invited to attend an ultrasound 'health-check' clinic. This paper provides a narrative account of the scanning procedure and operation of the service, with descriptive statistical analysis of GIs who attended. The analysis uses a structured, specially-developed clinical data set that incorporates a categorisation for the severity of FV damage. Case studies using ultrasound images and a link to a video are provided to illustrate the range of presentations encountered and the categorisations used for severity.
Results: A total of 160 groin scans (76 bilateral and 8 unilateral) were performed in 84 GIs. The majority were men (69.0%) and the mean age of the sample was 36.8 years. The mean duration of drug use and injecting drug use was 19.7 years and 13.8 years, respectively. FV damage at the injecting site in the right groin was graded as minimal in 20 patients (25%), moderate in 27 (33.8%), severe in 16 (20.0%) and very-severe in 17 (21.3%). Corresponding figures for left FV were 24 (30.0%), 22 (27.5%), 18 (22.5%) and 16 (20.0%). Wide variation was observed in the time to the development of these grades of FV damage.
Conclusions: Modern, portable ultrasound scanners make it possible to examine the venous health of GIs in community treatment settings. Ultrasound scanning identified extensive FV damage, much hitherto-unrecognised in this population. These findings should further alert clinicians, policy-makers and patients to the urgent need for effective harm reduction responses to GI behaviour. Images of damaged FV in this paper might prove to be a useful resource for discussions about GI risks.
Figures


References
-
- Hay G, Gannon M, MacDougall J, Millar T, Eastwood C, McKeganey N, L G. In: Measuring different aspects of problem drug use: Methodological developments. Singleton N, Murray R, L T, editor. London: Home Office; 2006. Local and national estimates of the prevalence of opiate use and/or crack cocaine use (2004/05)
-
- Rhodes T, Stoneman A, Hope V, Hunt N, Martin A, Judd A. Groin injecting in the context of crack cocaine and homelessness: From 'risk boundary' to 'acceptable risk'? Int J Drug Policy. 2006;17:164–170. doi: 10.1016/j.drugpo.2006.02.011. - DOI
-
- Williams K, Abbey E. Knowledge of deep vein thrombosis among intravenous drug misusers. Psychiatric Bulletin. 2006;30:263–265. doi: 10.1192/pb.30.7.263. - DOI
LinkOut - more resources
Full Text Sources
