

Recovery of urinary function after radical prostatectomy: predictors of urinary function on preoperative prostate magnetic resonance imaging
- PMID: 22264458
- PMCID: PMC4768862
- DOI: 10.1016/j.juro.2011.10.143
Recovery of urinary function after radical prostatectomy: predictors of urinary function on preoperative prostate magnetic resonance imaging
Abstract
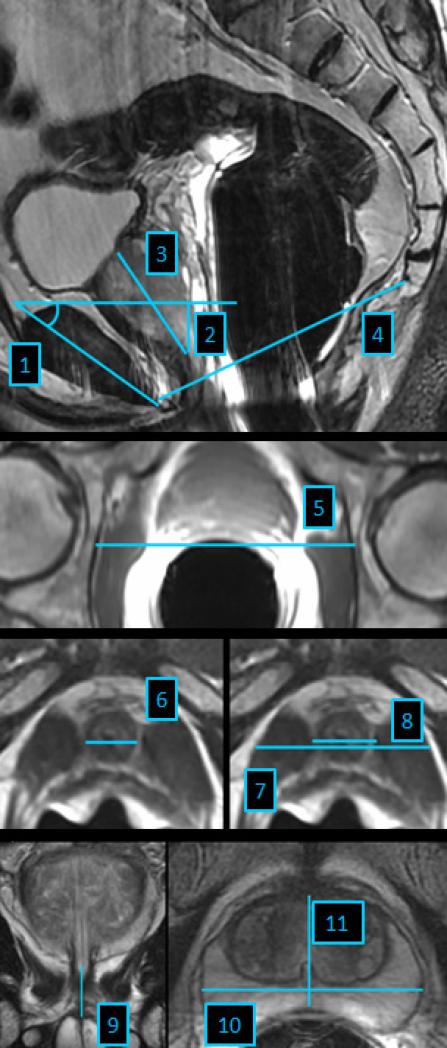
Purpose: We determined whether pelvic soft tissue and bony dimensions on endorectal magnetic resonance imaging influence the recovery of continence after radical prostatectomy, and whether adding significant magnetic resonance imaging variables to a statistical model improves the prediction of continence recovery.
Materials and methods: Between 2001 and 2004, 967 men undergoing radical prostatectomy underwent preoperative magnetic resonance imaging. Soft tissue and bony dimensions were retrospectively measured by 2 raters blinded to clinical and pathological data. Patients who received neoadjuvant therapy, who were preoperatively incontinent or had missing followup for continence were excluded from study, leaving 600 patients eligible for analysis. No pad use defined continent. Logistic regression was used to identify variables associated with continence recovery at 6 and 12 months. We evaluated whether the predictive accuracy of a base model was improved by adding independently significant magnetic resonance imaging variables.
Results: Urethral length and urethral volume were significantly associated with the recovery of continence at 6 and 12 months. Larger inner and outer levator distances were significantly associated with a decreased probability of regaining continence at 6 or 12 months, but they did not reach statistical significance for other points. Addition of these 4 magnetic resonance imaging variables to a base model including age, clinical stage, prostate specific antigen and comorbidities marginally improved the discrimination (12-month AUC improved from 0.587 to 0.634).
Conclusions: Membranous urethral length, urethral volume, and an anatomically close relation between the levator muscle and membranous urethra on preoperative magnetic resonance imaging are independent predictors of continence recovery after radical prostatectomy. The addition of magnetic resonance imaging variables to a base model improved the predictive accuracy for continence recovery, but the predictive accuracy remains low.
Copyright © 2012 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Can we better predict and treat urinary incontinence after prostatectomy?J Urol. 2012 Mar;187(3):789-90. doi: 10.1016/j.juro.2011.12.027. Epub 2012 Jan 15. J Urol. 2012. PMID: 22248524 No abstract available.
References
-
- Penson DF, McLerran D, Feng Z, et al. 5-year urinary and sexual outcomes after radical prostatectomy: results from the prostate cancer outcomes study. J Urol. 2005;173:1701. - PubMed
-
- Eastham JA, Kattan MW, Rogers E, et al. Risk factors for urinary incontinence after radical prostatectomy. J Urol. 1996;156:1707. - PubMed
-
- Sandhu JS, Eastham JA. Factors predicting early return of continence after radical prostatectomy. Curr Urol Rep. 2010;11:191. - PubMed
-
- Walsh PC, Donker PJ. Impotence following radical prostatectomy: insight into etiology and prevention. J Urol. 1982;128:492. - PubMed
-
- Budaus L, Isbarn H, Schlomm T, et al. Current technique of open intrafascial nerve- sparing retropubic prostatectomy. Eur Urol. 2009;56:317. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
