

Computational modeling of pancreatic cancer reveals kinetics of metastasis suggesting optimum treatment strategies
- PMID: 22265421
- PMCID: PMC3289413
- DOI: 10.1016/j.cell.2011.11.060
Computational modeling of pancreatic cancer reveals kinetics of metastasis suggesting optimum treatment strategies
Abstract
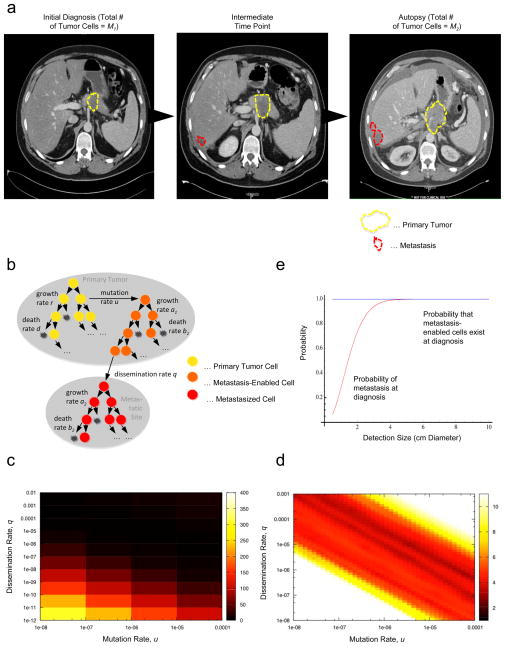
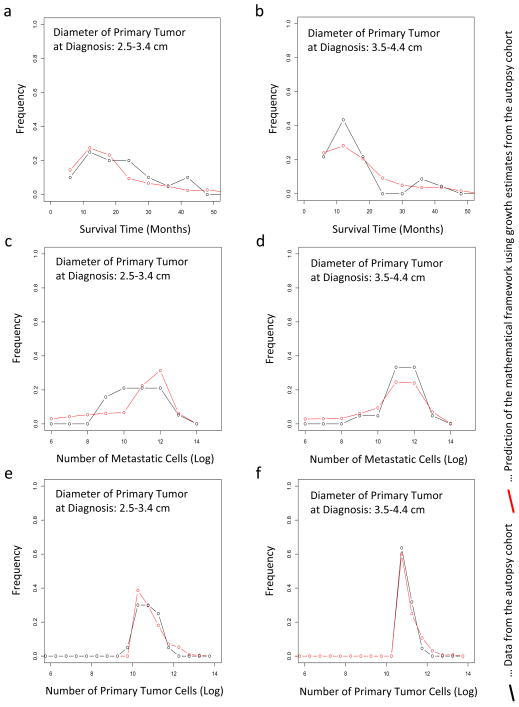
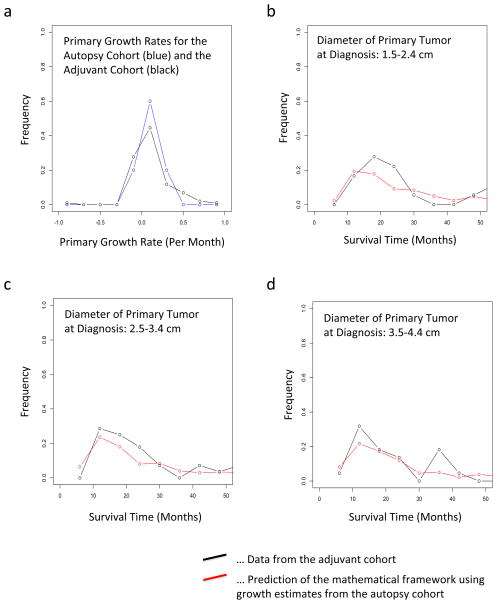
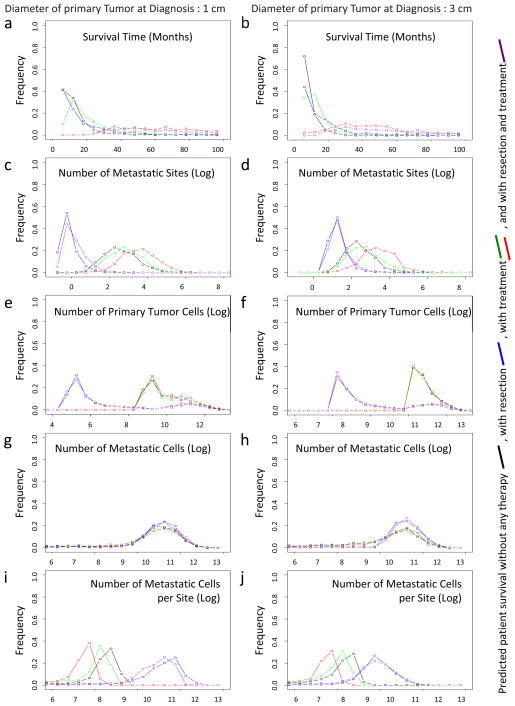
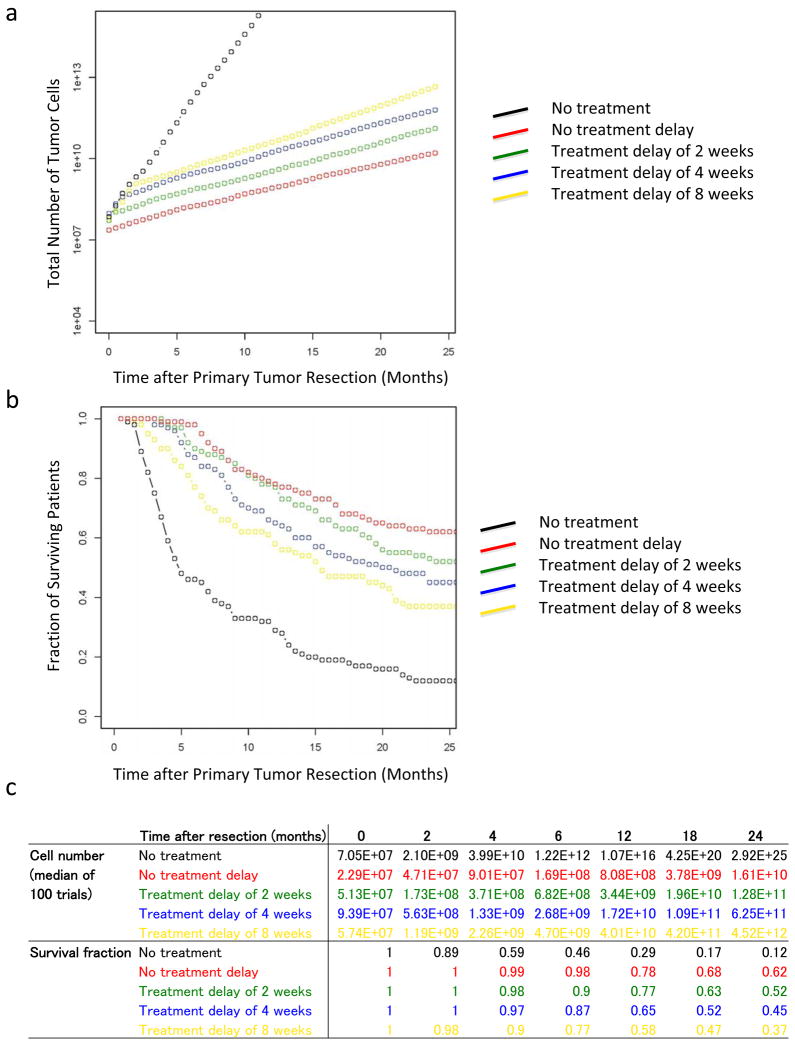
Pancreatic cancer is a leading cause of cancer-related death, largely due to metastatic dissemination. We investigated pancreatic cancer progression by utilizing a mathematical framework of metastasis formation together with comprehensive data of 228 patients, 101 of whom had autopsies. We found that pancreatic cancer growth is initially exponential. After estimating the rates of pancreatic cancer growth and dissemination, we determined that patients likely harbor metastases at diagnosis and predicted the number and size distribution of metastases as well as patient survival. These findings were validated in an independent database. Finally, we analyzed the effects of different treatment modalities, finding that therapies that efficiently reduce the growth rate of cells earlier in the course of treatment appear to be superior to upfront tumor resection. These predictions can be validated in the clinic. Our interdisciplinary approach provides insights into the dynamics of pancreatic cancer metastasis and identifies optimum therapeutic interventions.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Understanding metastasis in pancreatic cancer: a call for new clinical approaches.Cell. 2012 Jan 20;148(1-2):21-3. doi: 10.1016/j.cell.2011.12.021. Cell. 2012. PMID: 22265397
-
Navigating uncharted territory.Nat Rev Cancer. 2012 Feb 9;12(3):151. doi: 10.1038/nrc3229. Nat Rev Cancer. 2012. PMID: 22318236 No abstract available.
References
-
- Amikura K, Kobari M, Matsuno S. The time of occurrence of liver metastasis in carcinoma of the pancreas. Int J Pancreatol. 1995;17:139–146. - PubMed
-
- Andasari V, Gerisch A, Lolas G, South AP, Chaplain MA. Mathematical modeling of cancer cell invasion of tissue: biological insight from mathematical analysis and computational simulation. J Math Biol. 2011;63:141–171. - PubMed
-
- Artinyan A, Anaya DA, McKenzie S, Ellenhorn JD, Kim J. Neoadjuvant therapy is associated with improved survival in resectable pancreatic adenocarcinoma. Cancer. 2011;117:2044–2049. - PubMed
-
- Ayoub JP, Hess KR, Abbruzzese MC, Lenzi R, Raber MN, Abbruzzese JL. Unknown primary tumors metastatic to liver. J Clin Oncol. 1998;16:2105–2112. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
