

Trends in acute nonvariceal upper gastrointestinal bleeding in dialysis patients
- PMID: 22266666
- PMCID: PMC3294302
- DOI: 10.1681/ASN.2011070658
Trends in acute nonvariceal upper gastrointestinal bleeding in dialysis patients
Abstract
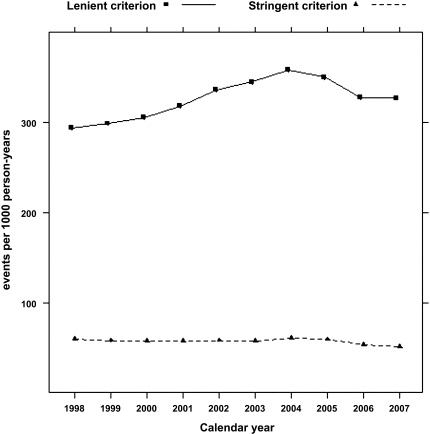
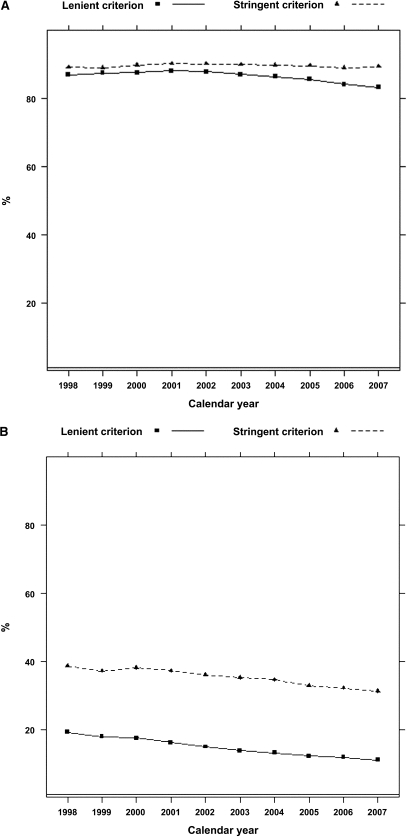
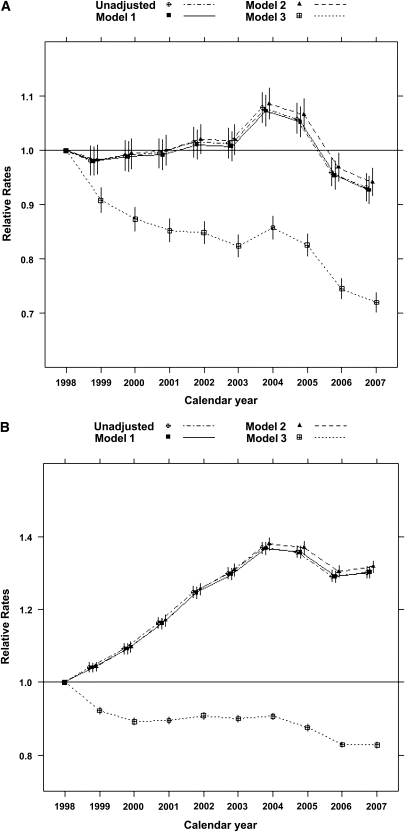
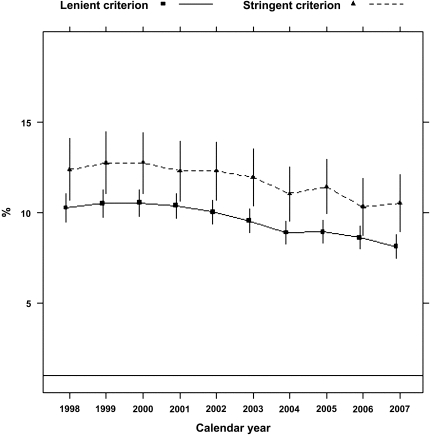
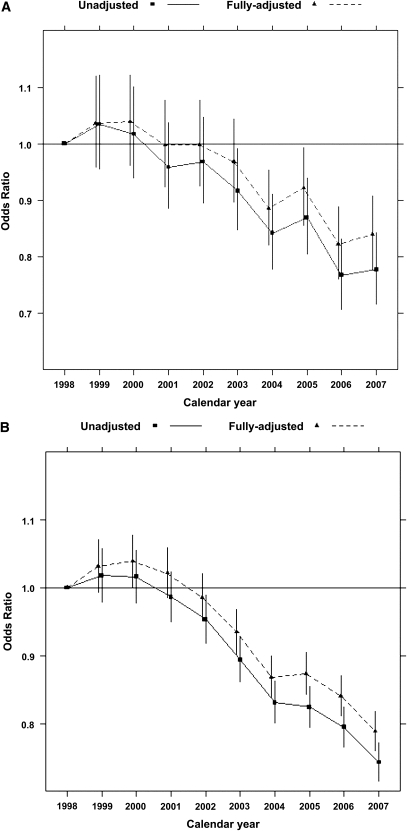
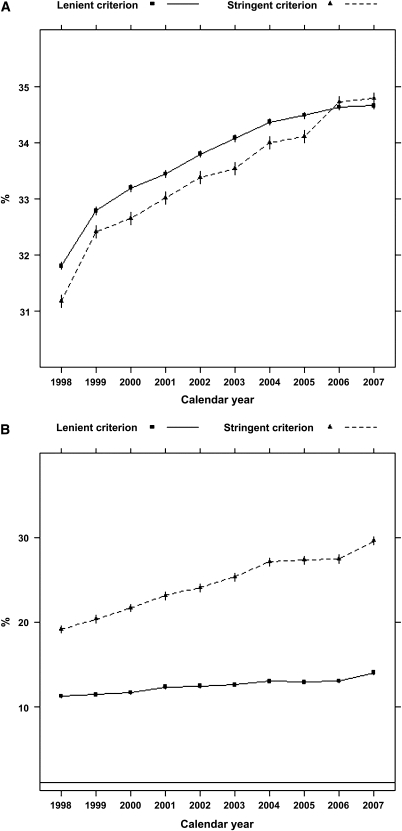
Impaired kidney function is a risk factor for upper gastrointestinal (GI) bleeding, an event associated with poor outcomes. The burden of upper GI bleeding and its effect on patients with ESRD are not well described. Using data from the US Renal Data System, we quantified the rates of occurrence of and associated 30-day mortality from acute, nonvariceal upper GI bleeding in patients undergoing dialysis; we used medical claims and previously validated algorithms where available. Overall, 948,345 patients contributed 2,296,323 patient-years for study. The occurrence rates for upper GI bleeding were 57 and 328 episodes per 1000 person-years according to stringent and lenient definitions of acute, nonvariceal upper GI bleeding, respectively. Unadjusted occurrence rates remained flat (stringent) or increased (lenient) from 1997 to 2008; after adjustment for sociodemographic characteristics and comorbid conditions, however, we found a significant decline for both definitions (linear approximation, 2.7% and 1.5% per year, respectively; P<0.001). In more recent years, patients had higher hematocrit levels before upper GI bleeding episodes and were more likely to receive blood transfusions during an episode. Overall 30-day mortality was 11.8%, which declined significantly over time (relative declines of 2.3% or 2.8% per year for the stringent and lenient definitions, respectively). In summary, despite declining trends worldwide, crude rates of acute, nonvariceal upper GI bleeding among patients undergoing dialysis have not decreased in the past 10 years. Although 30-day mortality related to upper GI bleeding declined, perhaps reflecting improvements in medical care, the burden on the ESRD population remains substantial.
Figures
References
-
- United States Renal Data System: USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2010
-
- Cheung J, Yu A, LaBossiere J, Zhu Q, Fedorak RN: Peptic ulcer bleeding outcomes adversely affected by end-stage renal disease. Gastrointest Endosc 71: 44–49, 2010 - PubMed
-
- Chiu PW, Ng EK: Predicting poor outcome from acute upper gastrointestinal hemorrhage. Gastroenterol Clin North Am 38: 215–230, 2009 - PubMed
-
- Wu CY, Wu MS, Kuo KN, Wang CB, Chen YJ, Lin JT: Long-term peptic ulcer rebleeding risk estimation in patients undergoing haemodialysis: A 10-year nationwide cohort study. Gut 60: 1038–1042, 2011 - PubMed
-
- Chiu PW, Sung JJ: Acute nonvariceal upper gastrointestinal bleeding. Curr Opin Gastroenterol 26: 425–428, 2010 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
