

Screening for gestational diabetes mellitus: are the criteria proposed by the international association of the Diabetes and Pregnancy Study Groups cost-effective?
- PMID: 22266735
- PMCID: PMC3322683
- DOI: 10.2337/dc11-1643
Screening for gestational diabetes mellitus: are the criteria proposed by the international association of the Diabetes and Pregnancy Study Groups cost-effective?
Abstract
Objective: The International Association of the Diabetes and Pregnancy Study Groups (IADPSG) recently recommended new criteria for diagnosing gestational diabetes mellitus (GDM). This study was undertaken to determine whether adopting the IADPSG criteria would be cost-effective, compared with the current standard of care.
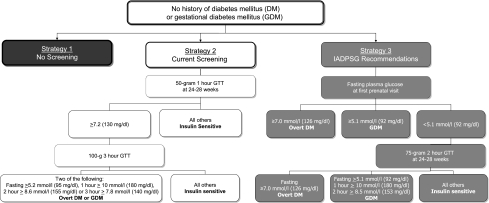
Research design and methods: We developed a decision analysis model comparing the cost-utility of three strategies to identify GDM: 1) no screening, 2) current screening practice (1-h 50-g glucose challenge test between 24 and 28 weeks followed by 3-h 100-g glucose tolerance test when indicated), or 3) screening practice proposed by the IADPSG. Assumptions included that 1) women diagnosed with GDM received additional prenatal monitoring, mitigating the risks of preeclampsia, shoulder dystocia, and birth injury; and 2) GDM women had opportunity for intensive postdelivery counseling and behavior modification to reduce future diabetes risks. The primary outcome measure was the incremental cost-effectiveness ratio (ICER).
Results: Our model demonstrates that the IADPSG recommendations are cost-effective only when postdelivery care reduces diabetes incidence. For every 100,000 women screened, 6,178 quality-adjusted life-years (QALYs) are gained, at a cost of $125,633,826. The ICER for the IADPSG strategy compared with the current standard was $20,336 per QALY gained. When postdelivery care was not accomplished, the IADPSG strategy was no longer cost-effective. These results were robust in sensitivity analyses.
Conclusions: The IADPSG recommendation for glucose screening in pregnancy is cost-effective. The model is most sensitive to the likelihood of preventing future diabetes in patients identified with GDM using postdelivery counseling and intervention.
Figures
Comment in
-
Gestational diabetes mellitus: implications of an increased frequency with IADPSG criteria.Diabetes Care. 2012 Mar;35(3):461-2. doi: 10.2337/dc11-2237. Diabetes Care. 2012. PMID: 22355016 Free PMC article. No abstract available.
References
-
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins--Obstetrics. ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists. Number 30, September 2001 (replaces Technical Bulletin Number 200, December 1994). Gestational diabetes. Obstet Gynecol 2001;98:525–538 - PubMed
-
- Metzger BE, Lowe LP, Dyer AR, et al. ; HAPO Study Cooperative Research Group. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 2008;358:1991–2002 - PubMed
-
- Landon MB, Mele L, Spong CY, et al. ; Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units (MFMU) Network. The relationship between maternal glycemia and perinatal outcome. Obstet Gynecol 2011;117:218–224
-
- Xiong X, Saunders LD, Wang FL, Demianczuk NN. Gestational diabetes mellitus: prevalence, risk factors, maternal and infant outcomes. Int J Gynaecol Obstet 2001;75:221–228 - PubMed
-
- Ray JG, Vermeulen MJ, Shapiro JL, Kenshole AB; Diabetes Endocrine Pregnancy Outcome Study in Toronto. Maternal and neonatal outcomes in pregestational and gestational diabetes mellitus, and the influence of maternal obesity and weight gain: the DEPOSIT study. QJM 2001;94:347–356 - PubMed
