

Management of bleeding and artificial gastric ulcers associated with endoscopic submucosal dissection
- PMID: 22267977
- PMCID: PMC3262173
- DOI: 10.4253/wjge.v4.i1.1
Management of bleeding and artificial gastric ulcers associated with endoscopic submucosal dissection
Abstract
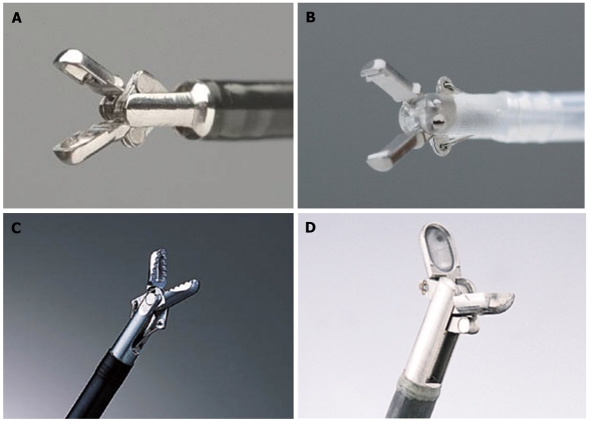
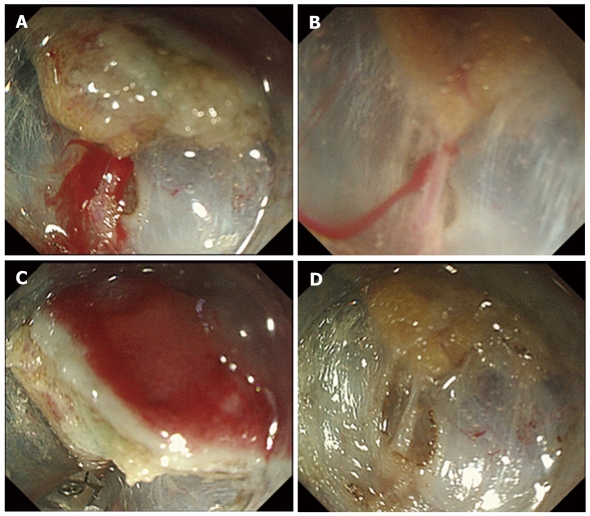
Endoscopic submucosal dissection (ESD), an endoscopic procedure for the treatment of gastric epithelial neoplasia without lymph node metastases, spread rapidly, primarily in Japan, starting in the late 1990s. ESD enables en bloc resection of lesions that are difficult to resect using conventional endoscopic mucosal resection (EMR). However, in comparison to EMR, ESD requires a high level of endoscopic competence and a longer resection time. Thus, ESD is associated with a higher risk of adverse events, including intraoperative and postoperative bleeding and gastrointestinal perforation. In particular, because of a higher incidence of intraoperative bleeding with mucosal incision and submucosal dissection, which are distinctive endoscopic procedures in ESD, a strategy for endoscopic hemostasis, mainly by thermo-coagulation hemostasis using hemostatic forceps, is important. In addition, because of iatrogenic artificial ulcers that always form after ESD, endoscopic hemostasis and appropriate pharmacotherapy during the healing process are essential.
Keywords: Artificial ulcer; Endoscopic hemostasis; Endoscopic submucosal dissection; Gastric epithelial neoplasia; Hemostatic forceps.
Figures
References
-
- Ohkuwa M, Hosokawa K, Boku N, Ohtu A, Tajiri H, Yoshida S. New endoscopic treatment for intramucosal gastric tumors using an insulated-tip diathermic knife. Endoscopy. 2001;33:221–226. - PubMed
-
- Gotoda T. A large endoscopic resection by endoscopic submucosal dissection procedure for early gastric cancer. Clin Gastroenterol Hepatol. 2005;3:S71–S73. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
