

Review
doi: 10.3174/ajnr.A2899.
Epub 2012 Jan 19.
Intrathecal gadolinium-enhanced MR cisternography: a comprehensive review
Affiliations
- PMID: 22268089
- PMCID: PMC7966334
- DOI: 10.3174/ajnr.A2899
Item in Clipboard
Review
Intrathecal gadolinium-enhanced MR cisternography: a comprehensive review
AJNR Am J Neuroradiol.
2013 Jan.
Abstract
CE-MRC has been in use for the past 15 years and was reported to be a useful method in the evaluation of CSF disorders and hydrocephalus. The use of CE-MRC in conjunction with other MR imaging techniques has been shown to be effective in selected cases for the evaluation of several disorders of cerebrospinal system. CE-MRC has certain advantages over other cisternographic studies with fewer side effects if performed properly. Although intrathecal Gd administration is not widely accepted yet, several recent studies have reported the safety of small-dose intrathecal gadolinium injection. In this review, we describe CE-MRC and review recent applications in several clinical conditions.
Figures
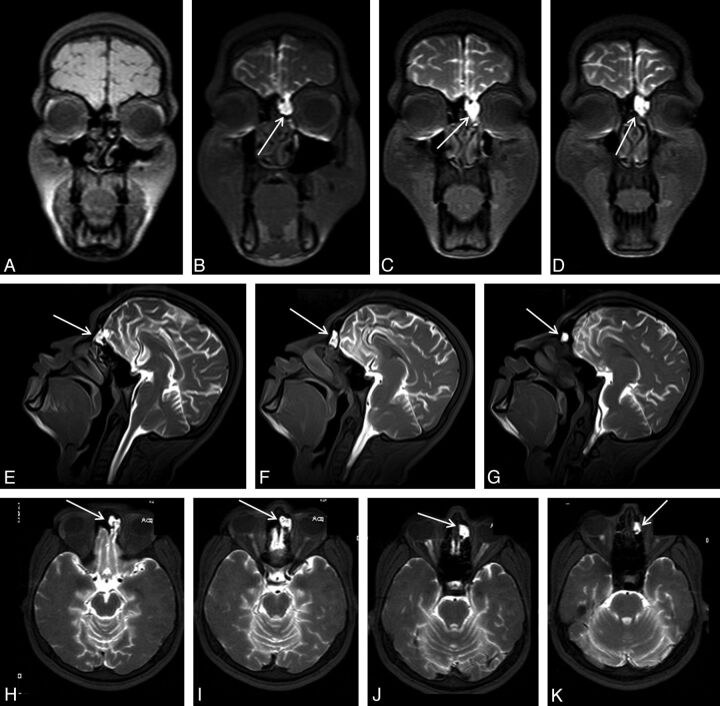
An 18-year-old man with posttraumatic recurrent meningitis. Coronal precontrast T1WI shows irregularity and heterogeneity of the left cribriform plate (A). Early-phase postcontrast T1WI demonstrates passage of the contrast material from left cribriform plate through anterior ethmoid cells (arrows in B-K). Presence of the left cribriform plate defect was confirmed at surgery.

A 42-year-old man with spontaneous intracranial hypotension syndrome. Postcontrast early-phase sagittal (left) and coronal (right) T1WI shows leakage of contrast material into the paraspinal space at the thoracolumbar junction level (arrows). In this patient, epidural blood patch was planned.
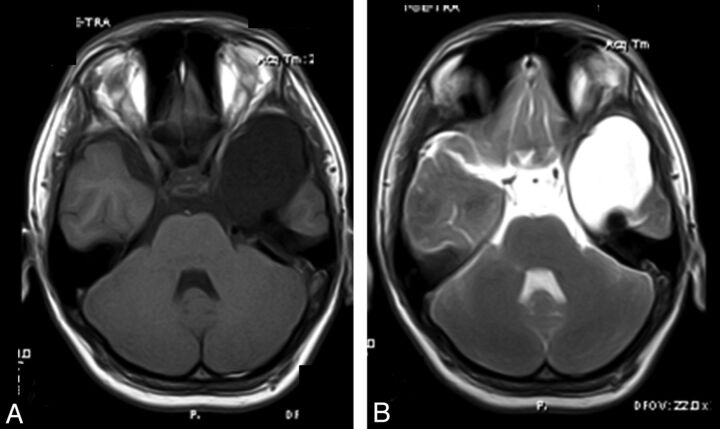
A 17-year-old boy with syncope history. Axial precontrast (A) and early-phase postcontrast (B) T1WI. Axial postcontrast T1WI shows opacification of the arachnoid cyst in the left temporal fossa (B) consistent with a communicating type temporal arachnoid cyst.
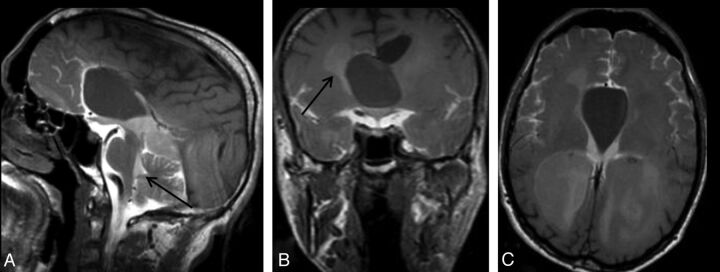
A 34-year-old man with headache. Sagittal early-phase postcontrast T1WI reveals an arachnoid cyst at the septum pellicidum (A). Early-phase postcontrast T1WI shows passage of the intrathecally administered contrast to the fourth ventricle (arrow) and basal cisterns, whereas there is no contrast in the arachnoid cyst (A). Coronal (B) and axial (C) late-phase postcontrast images show passage of the contrast to the lateral ventricles (arrow in B), but not to the arachnoid cyst. Imaging findings are consistent with a non-communicating arachnoid cyst.
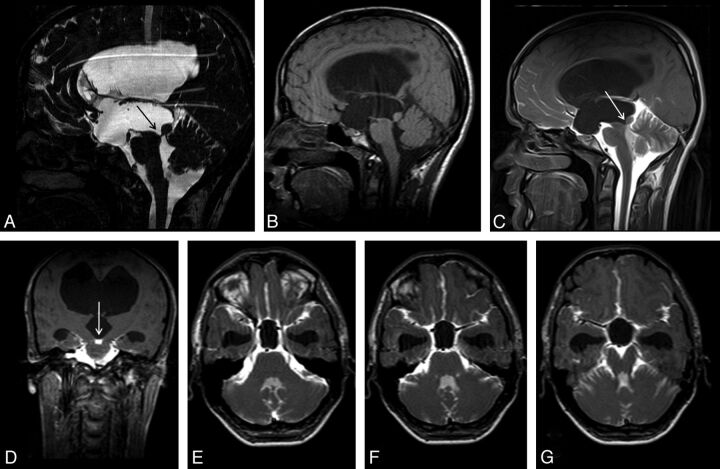
A 20-year-old man with headache. Sagittal 3D-CISS (A) and precontrast T1WI (B) shows hydrocephalus. Sagittal 3D-CISS image demonstrates a linear hypointense band at the cerebral aqueduct (arrow in A). The inferior wall of the third ventricle cannot be depicted clearly on 3D-CISS image (A). Early-phase postcontrast sagittal and coronal T1WI shows passage of the intrathecally administered contrast to the fourth ventricle, but not to the third ventricle (arrows) (C, D). Imaging findings are consistent with aqueductal stenosis and hydrocephalus secondary to a web. A 12-hour post injection axial sequential T1WI showed no relation between the basal cisterns and the third ventricle (E-G). The intact third ventricular floor implies absence of a STV, and tells us ETV or shunt procedures are necessary.
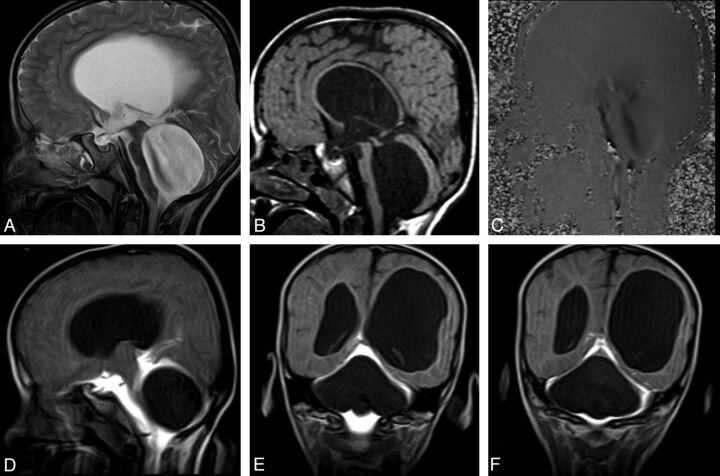
A 6-year-old boy with headache and syncope. Sagittal T2WI (A) and precontrast T1WI (B) show enlargement of the third and fourth ventricles with flattening of the corpus callosum. Sagittal PC-MR image demonstrates the black-coded flow at anterior fourth ventricle (C). Early-phase postcontrast T1WI clearly shows a non-communicating type cystic lesion leading to fourth ventricle enlargement (D-F).
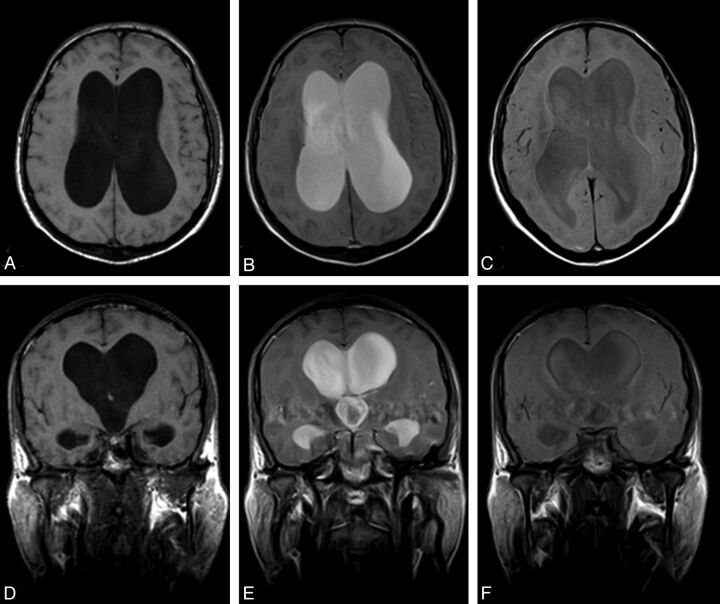
Positive CE-MRC examination of a 67-year-old woman with definite NPH. Axial (A) and coronal (D) precontrast T1WI shows ventriculomegaly and effacement of the cisterns at convexity level. After intrathecal Gd-DTPA injection, the contrast material persisted in the lateral ventricles at 24 (B, E) and 48 (C, F) hours.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous